










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.31 no.4 Lisboa dez. 2017
REVIEW ARTICLE
The role of bone biomarkers and new imaging techniques in the management of patients with CKD-MBD
C Belino1, C Meng2,4-7, L Pereira2,4-7, C Carvalho3-6, R Neto2,4-7
1 Serviço de Nefrologia, Centro Hospitalar Vila Nova de Gaia e Espinho, Vila Nova de Gaia, Portugal
2 Serviço de Nefrologia, Hospital de São João, Porto, Portugal
3 Serviço de Nefrologia, Hospital de Braga, Braga, Portugal
4 Laboratório de Histomorfometria Óssea do Hospital de São João
5 Instituto de Investigação e Inovação em Saúde, Universidade do Porto, Porto, Portugal
6 INEB, Instituto Nacional de Engenharia Biomédica, Universidade do Porto, Porto, Portugal
7 Departamento de Medicina Interna, Faculdade de Medicina da Universidade do Porto
ABSTRACT
Chronic kidney Disease – Mineral and Bone Disorder (CKD-MBD) encompasses abnormalities in bone turnover, volume and mineralization, compromising bone quantity and quality. Bone biopsy is the gold standard to access bone changes, but is not available in many centers and neither is it included in routine practice. The need for a noninvasive method to evaluate bone disease has promoted the development of multiple bone biomarkers and imaging techniques to assess bone metabolism, to clarify the risk of bone loss and fractures and to guide therapeutic decisions. However, all of these have important limitations and presently no noninvasive method either isolated or in association can replace bone biopsy. This article will discuss the major groups of bone biomarkers and new imaging techniques and their role in CKD-MBD.
Key-words: CKD-MBD, bone disease, bone biomarkers, imaging techniques.
INTRODUCTION
Chronic kidney Disease – Mineral and Bone Disorder (CKD-MBD) is a syndrome characterized by abnormalities in mineral and bone metabolism. This entity often promotes vascular calcifications, increases cardiovascular mortality and predisposes to a higher risk of fractures. Therefore, it is related with poor outcomes in chronic kidney disease (CKD) patients and early recognition and management are crucial for a better prognosis. Bone biopsy is the gold standard for diagnosis and classification of bone disorders. However, this procedure is not feasible for all patients.
The necessity for a noninvasive method to evaluate bone disease has promoted the development of multiple bone biomarkers and imaging techniques to assess bone metabolism, to clarify the risk of bone loss and fractures and to guide therapeutic decisions1-4. However, all these have limitations in the assessment of bone disease and presently no noninvasive method either isolated or in association can replace bone biopsy1-3. In this article we will review the current role of major bone biomarkers and bone assessment image techniques.
BONE BIOMARKERS
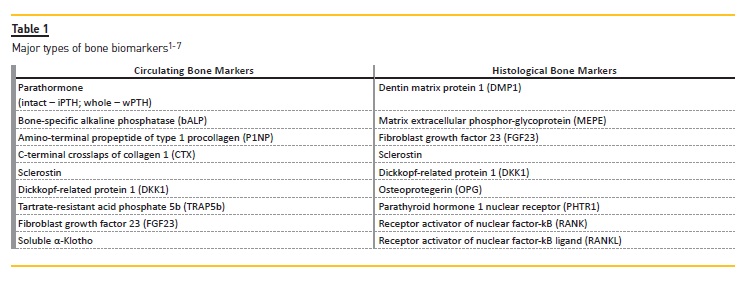
Bone biomarkers can be divided into two major groups: circulating markers and markers available in situ by immunochemistry analysis of undecalcified bone1,2.
Circulating biomarkers are those which can reflect and/or affect bone turnover. Histological markers reflect bone cell number and/or activity. Table 1 summarizes the major markers of both groups.
Biochemical markers reveal changes in bone turnover more rapidly than other clinical or imaging tests and they can reflect the acute effects of disease and therapy. They also represent the skeleton as a whole, whereas histomorphometric indices reflect its activation at a definite site. The ease of sample collection is also an important advantage. However, the high intra and inter-individual variability, lack of tissue specificity, accumulation in renal and/or hepatic failure, short halflife and circadian rhythm are important limitations. Age, ethnicity, geographic location and effects of therapy, especially dialysis (some may be dialyzable) can affect results and more data are needed4.
Circulating Bone Markers
Parathormone (PTH)was the first biomarker identified that showed good correlation with bone histomorphometric parameters. However, the first studies used a now unavailable first-generation immunoradiometric assay (Allegro PTH assay) and KDIGO recommendations for PTH range target were based on values retrieved with this assay1. Studies from the past 15 years using second-generation (intact PTH – iPTH) and third-generation assays (biointact – biPTH; 1-84 PTH) have shown a week correlation between PTH levels and bone turnover except at extremes of the PTH concentration range1,8,9. By current guidelines8,9, PTH has not proven to be specific or sensitive enough to accurately diagnose bone disease. Variation of PTH levels may occur with advanced age, gender, comorbidities and can be associated with the short half-life of the whole active hormone (which can increase by 25% in dialysis patients)1,10.
Furthermore, there are differences according to antibody specificity, standardization methods, temperature, the speed of sample processing and type of preservative used in samples collected1. Biological activity is affected by several factors, such as oxidation, chronic inflammation, competing downstream signals, inhibitory local factors and uremic toxins, which suppress bone response and produce what has been called PTH resistance, now considered PTH hyporesponsiveness4. This may help to explain the higher prevalence of adynamic bone disease, even in advanced stages of CKD, where PTH levels are usually higher4.
Considering this, the new 2017 KDIGO guidelines on management of CKD-MBD recommend that patients in stages G3a-G5 not on dialysis with intact PTH levels progressively rising or persistently above the upper normal limit for the assay should be evaluated for modifiable factors, including hyperphosphatemia, hypocalcemia, high phosphate intake and vitamin D deficiency (2C)9.
There are no ideal PTH range values. Regarding dialysis patients, a study with one of the largest cohorts (492 patients) documented an optimal iPTH level to discriminate low from non-low turnover disease of 104 pg/mg and high versus non-high turnover disease of 323 pg/ml. However, using the 2009 KDIGO PTH values of greater than 2 but less than 9 times the upper limit of normal, sensitivity and specificity of iPTH level to discriminate low from non-low turnover disease were 65.7% and 65.3%, and to discriminate high from non-high disease were 37.0% and 85.8%. No further conclusion was obtained from posterior studies so the recommendation remained the same in the new guidelines9.
Bone-specific alkaline phosphatase (bALP) is an osteoblast enzyme that promotes mineralization. There are at least 4 isoforms of bALP: B/I, B1, B2 and BX14.
The bone isoform accounts for about a half of all total circulating enzyme and the remaining mainly originates from hepatocytes, with cross-reactivity between bone and liver isoforms of 20%4. In the absence of cholestatic liver disease, total alkaline phosphatase levels reflect elevation of bALP, which is considered to reflect bone turnover4,8. Current evidence shows a borderline usefulness for its application, with best cut-off of 33.1 U/L for low versus non-low turnover and 42.1 U/L for high versus non-high turnover11. This enzyme was only slightly better than PTH for diagnosing low-turnover disease but not for high-turnover disease. Also, results did not support the combined use of bALP and PTH11-14. However, bALP can be useful. The predictive value for low-turnover disease can be increased by applying a lower cut-off value for bALP and the same is true for high-turnover disease, by using a higher cut-off value above 42.1 U/L. Small recent studies showed that bALP isoform BX1 significantly improved the diagnostic accuracy for low-turnover disease3. Therefore, there is still a chance of a promising role for bALP in CKD-MBD management. KDIGO new guidelines still recommend the monitoring of serum ALP beginning in CKD stage 3 and every 12 months in stages 4-5D or more frequently in the presence of elevated PTH (not graded)8,9.
Osteocalcin is a protein secreted to circulation by osteoblasts during bone turnover and has a significant correlation with histomorphometric parameters of bone. Despite being a weaker predictor than bALP, osteocalcin was superior to iPTH for detecting adynamic bone disease12,14. However, a high analytical variability and uremic retention hampers its widespread use as a bone biomarker4.
Amino-terminal (N-terminal and C-terminal) propeptides of type 1 procollagen (P1NP) are collagen fragments released to circulation during bone maturation and are indicative of collagen rate formation4,8. The monomeric form accumulates in CKD. P1NP was outperformed by iPTH and bALP in detection of low versus non-low turnover disease and had no additional value over iPTH for detection of high-turnover disease11. They are not currently used for clinical purposes.
C-terminal crosslaps of collagen 1 (CTX) is the carboxy-terminal telopeptide of type I collagen and is usually produced during matrix degradation in bone reabsorption3.
The International Osteoporosis Foundation has recommended that serum CTX-I levels be used as reference marker for bone resorption. However, telopetides are retained in renal failure and have an important circadian rhythm so they cannot be recommended as bone biomarkers in CKD4. Bone biopsy studies evaluating the utility of CTX-I are limited and overall had disappointing results4.
Tartrate-resistant acid phosphate 5b (TRAP5b) is a major enzyme released by osteoclasts during bone reabsorption. Levels of TRAP5b correlated highly with bone turnover; a sensitive and specific marker of osteoclast activity. Similar to bALP, levels are not affected by renal or liver function, do not possess circadian rhythm and intra-individual variation is low, even in dialysis patients3,4. Studies are needed to evaluate the role of this biomarker in CKD patients.
Sclerostin is secreted by osteocytes and is an inhibitor of bone formation, correlating negatively with bone formation parameters. Levels rise early in CKD and increase progressively; two to four-hold higher in dialysis patients. Low levels were better predictors of low and high-turnover disease than iPTH4. Animal models with high skeletal and serum expression of sclerostin were associated with low-turnover disease in early CKD and this may account for the higher prevalence of adynamic bone disease in early CKD stages. The use of anti-sclerostin antibody increased bone volume and mineralization in animals with low PTH but not in high PTH12. A role in vascular calcifications and mortality is currently being studied15,16.
Dickkopf-related protein 1 (DKK1) is expressed by osteoblasts and osteocytes and is also a bone formation inhibitor. Data about the role of DKK1 in CKD are scarce and inconsistence. Behets et al.17 tried to describe for the first time the relationship between DKK1, sclerostin and laboratory parameters of mineral metabolism across stages of CKD, including dialysis. DKK1 was not increased in advanced stages of CKD. Levels were related with PTH (inverse relationship in dialysis patients),1, 25(OH) 2 vitamin D concentrations (inverse relationship in pre-dialysis patients) and phosphate (positive and independent association). Bone turnover markers were highest in hemodialysis patients presenting the combination of high PTH with low sclerostin level. The authors concluded that serum levels of DKK1 and sclerostin are unrelated, suggesting different sites of origin and/or regulatory mechanisms.
Fibroblast growth factor 23 (FGF-23) is a hormone secreted by osteoblasts and osteocytes that regulates phosphorus excretion by the kidneys and inhibits the formation of the active form of vitamin D. FGF-23 is a potentially relevant biomarker for CKD-MBD and has shown to be more sensitive and specific than PTH in earlier stages of CKD18. However, there is a lack of data regarding effects of lowering FGF-23 levels. Attempts to lower levels in animal models have resulted in increased vascular calcifications, hyperphosphatemia and excess mortality5. A link between higher FGF-23 concentrations and risk of cardiovascular events and mortality across the spectrum of CKD has been suggested in several studies but further clarification of this biomarker role is needed17.
α-soluble Klotho (sKl) is the less studied marker, intimately linked to phosphate metabolism. In CKD, sKL has shown inverse correlations with left ventricular dysfunction, carotid artery intimal thickness and arterial stiffness. An inverse association to mortality has been reported, with higher circulating levels associated with increased survival, even in dialysis patients, but more data are needed5.
Histological Bone Markers
The study of in situ expression of molecules in the bone allows a better understanding of the pathophysiology of CKD-MBD. There are numerous molecules already identified, however, due to lack of specificity and poorly understood underlying mechanisms, routine measure and monitoring are not yet clinically recommended2. The major aspects of these markers are summarized next.
Expression of sclerostin in trabecular bone surface of CKD patients was negatively correlated with bone formation rate. DKK1 seems to have similar effects. FGF23 and its co-receptor Klotho inhibited mineralization and osteoblast activity and were inversed correlated with static indices of osteoid mineralization, suggesting an accelerating effect on mineralization. PTHR1 functions as a receptor for PTH and PTH-related proteins in bone and is highly expressed in osteocytes in CKD. RANK is a member of the tumor necrosis factor receptor and activates multiple signals responsible for cell differentiation, function and survival and controls bone regeneration and remodeling. RANK and his ligand, RANKL, are essential for complete maturation, reabsorption activity and survival of osteoclasts. Osteoprotegerin (OPG) inhibits osteoclastogenesis, neutralizing the osteoclastic function induced by RANK/RANKL. RANKL/OPG ratio is an important determinant of bone mass and skeletal integrity. DMP1 has a high calcium ion-biding capacity and is involved in bone homeostasis2.
NEW IMAGING TECHNIQUES
Current techniques suited to be partial surrogates for mineralized bone histology are dual-energy X-ray absorptiometry (DXA) and quantitative computed tomography in its various forms (central, peripheral, high resolution (HR-pQCT) and microcomputed). Highresolution magnetic resonance imaging (HR-MRI or micro-MRI) also allows the non-invasive assessment of bone microstructure19,20.
Dual X-Ray Absorptiometry
DXA measures areal bone mineral density (BMD) using minimal radiation and rapid scan times with a good reproducibility and reliable ranges for age, gender and race21.
The application of DXA in chronic kidney disease (CKD) is complex because DXA only measures mineral content.
Completely different causes of renal osteodystrophy may lead to similar low values of BMD. Thus, high-turnover disease, low-turnover disease, age or sex-related osteoporosis may all show similar densitometric values22. DXA neither does not correlate with bone histology or histomorphometric analysis of bone activity and does not provide information about bone microarquitecture19-22.
Considering this, the 2009 KDIGO guidelines8 recommended DXA to assess fracture risk in patients with CKD stage 1 to early stage 3, as long as biochemical testing does not suggest CKD-MBD. Regarding more advanced stages, it was stated that In patients with CKD stages 3-5D with evidence of CKD-MBD, we suggest that BMD testing not be performed routinely because it has not been shown that BMD predicted fracture risk as it does in the general population, and BMD does not predict the type or renal osteodystrophy (2B). So the rational was that low BMD was probably due to CKD-MBD and controlling PTH and phosphorus loading were considered safer and appropriate than antiresorptive therapy. However, the majority of this evidence came from crosssectional studies.
More recently, prospective cohort studies have demonstrated that DXA predicted fractures also in CKD stages 3-5D. Naylor et al.23 evaluated the ability of FRAX (Fracture Risk Assessment Tool, which includes DXA data) to predict major osteoporotic fractures in 2017 adults ≥ 40 years of age (320 patients with a GFR < 60 ml/min/1.73m2) in the Canadian Multicenter Osteoporosis Study. FRAX with BMD, FRAX without BMD and the femoral neck T-score all predicted fractures, with best performance for femoral neck T-score with inclusion of fall history. Liomori et al.24 reported a significant correlation between DXA BMD values and fracture risk in a group of 485 elderly hemodialysis patients. The new 2017 KDIGO guidelines9 updated the recommendation to the following: In patients with CKD G3a-G5D with evidence of CKD-MBD and/or risk factors for osteoporosis, we suggest BMD testing to assess fracture risk if results will impact treatment decisions (2B).
Transplanted patients are even more complex, since bone arquitecture is additionally altered by such transplant-related factors as steroids and calcineurin inhibitors.
There are no prospective studies addressing the ability of DXA to predict fractures in transplant patients.
Few studies have compared BMD with histomorphometric data and those which did reveal an elevated prevalence of low-turnover disease and low bone volume in transplanted patients25,26. The 2009 KDIGO guidelines recommended BMD testing in the first 3 months following transplantation in patients with an GFR greater than 30 ml/min/1.73m2 if they receive steroids or have risk factors for osteoporosis but not recommended DXA for those with CKD G4T to G5T.
However, as previously demonstrated, there is growing evidence that DXA predicts fractures across the spectrum of CKD. The revised guideline9 statement recommends BMD testing in transplant recipients with CKD G1T-G5T with risk factors for osteoporosis if the results will impact treatment decisions (2C).
Trabecular Bone Score
Trabecular bone Score (TBS) is a measure of grey scale homogeneity from DXA spine scans and correlates with microarquitecture and fracture risk4. Evidence regarding TBS use in CKD is limited, but recent studies suggest a benefit to its use throughout different stages of CKD, with it possibly being more accurate for fracture risk assessment in the early stages of disease and in transplanted patients26,27. At this time, it is unclear if TBS can be an effective noninvasive tool in the assessment and management of bone disease in CKD patients.
This technique may correlate with other imaging methods but until the present has not been validated with underlying bone histology or activity so therapeutic changes based on it cannot be recommended21.
Quantitative Computerized Tomography Techniques
Quantitative Computerized Tomography (QTC) allows 3D cross-sectional imaging of the central and axial skeleton to provide spatial or volumetric BMD as well as distinction between cortical and trabecular compartments29.
There are few studies into the appliance of this technique in CKD but results are promising, showing a positive association between QTC measurements and histomorphometric analysis21,30.
Peripheral QTC (pQTC) minimizes the dose of ionizing radiation by focusing on the tibia and distal radius.
Studies in dialysis patients reported a significant association between an elevated fracture risk and decreases in distal radial cortical BMD, cortical area and thickness, torsional and bending strength31. These results supported the evidence that bone quality loss is associated with increased fracture risk in dialysis patients. Currently, pQTCs are not available for clinical purposes but promise to be an important tool in the future21.
High-Resolution Imaging
Only 70–75% of bone strength is explained by bone mineral density. The remaining 25–30% is explained by bone microarquitecture and tissue composition1. In the context of renal osteodystrophy, assessment of microdamage is fundamental for prognosis and therapeutic strategies. Currently, HR-pQTC and micro-MRI are the best techniques to achieve these requirements.
The structural parameters measured by these two techniques showed good correlation with histomorphometric parameters, leading some clinicians to refer to the process as a virtual bone biopsy. However, the high spatial resolution required to resolve bone microarquitecture in a feasible scan time is challenging and there are several limitations that presently impair the widespread use of this techniques19.
HR-pQTC uses a low-radiation scanner to measure cortical and trabecular bone structural parameters and volumetric BMD (vBMD) from distal radius and tibia. It has a greater resolution than pQTC and allows evaluation of trabecular microarchitecture in addition to the parameters measured by QCT and pQCT (21, 29). Few but increasing numbers of studies in CKD have been performed.
Hr-pQTC of the radius and tibia has been shown to differentiate between CKD patients with and without increased fracture risk29. However, the predictive power to individually detect fractures was low, improving slightly for patients with the longest duration of CKD. Current evidence does not show that the addition of pQTC or HR-pQTC parameters to DXA BMD improves fracture discrimination ability, but these techniques may play a particular role in monitoring patients with CKD19-21,32.
Micro-CT and Micro-MRI are techniques with resolution as low as 8 μm compared to 100 μm for HR-pQCT, providing similar results to an actual bone biopsy.
Micro-CT, while promising, is limited to in vitro and animal studies29. Micro-MRI is a non-ionizing method for in vivo quantification of bone microarquitecture from distal tibia, radius and femur. Trabecular orientation and structure are clearly elucidated. Multiple studies using micro-MRI in non-CKD patients found a correlation between bone structure and fracture discrimination and demonstrated structural and mechanical implications of therapeutic strategies longitudinally on bone33,34. Unfortunately, studies in CKD are very few. Disruption of trabecular network, lower cortical thickness and decreased stiffness and strength could be seen in dialysis and transplanted patients35,36.
At present, the availability of these techniques is extremely limited and further studies are necessary before widespread clinical use19,21.
Ultrashort-echo-time radial MRI imaging is a technique that quantifies bone water concentration as a marker of bone quality. Most bone water resides in the microscopic pores of the haversian and lacuno canalicular systems; cortical bone contains about 20% of water by volume. A small fraction of cortical water is bound to collagen and matrix substrate. The hydrated state of the bone is essential in conferring on bone material its unique viscoelastic properties. An increase in pore volume as result of age or increased bone turnover reduces mechanical competence of bone and increases water content37. Techawiboonwong et al.37 found increased porosity with bone water content 135% higher in hemodialysis patients compared to pre-menopausal women with normal renal function, despite no significant differences in vBMD of both groups. The utility of this technique in CKD patients is still to be clarified.
High-resolution MRI (HR-MRI) constructs 3D images of bone geometry and trabecular microarquitecture at peripheral sites with no use of ionizing radiation. Link et al.38 analyzed trabecular bone structure of the calcaneus in a group of transplanted patients and concluded that HR-MRI images may be used to characterize fracture incidence in this patient group. Further studies are needed to clarify the role of this technique across the spectrum of CKD.
Finite Element Analysis is a computational method that provides estimates of bone stiffness and failure load after stimulation with mechanical loads and can be applied to both HR-pQTC and HI-MRI to measure strength of whole bone or its compartments19. It also provides additional information on fragility and fracture risk, independent of BMD or architecture measurements; another potential method of assessing bone vulnerability19. This is another promising method for further future studies, particularly relevant in patients with advanced CKD and high rates of hip fractures19.
CONCLUSIONS
There is a weak correlation between PTH values and bone turnover, especially for high-turnover disease.
Extremes of the PTH concentration range better predicted turnover. Other circulating bone markers such as bALP, FGF-23 or sclerostin can help to improve the predictive value of PTH. Understanding the role of bone biomolecules in CKD-MBD may have future implications in therapeutic strategies because they may reflect an ongoing process before changes occur in histomorphometric analysis or analytical parameters. In situ markers are essential to understand the pathophysiology of CKD-MBD. Noninvasive imaging techniques have the potential to complement bone biomarkers in the assessment and monitoring of CKD-MBD, screening of bone fragility and fracture risk and development of new therapeutic approaches. However, this additive value over biomarkers has not yet been proven and imaging techniques do not give cellular, biochemical and composition information. Solid evidence regarding the benefit of imaging techniques use in CKD is lacking, with exception of DXA. Elevated costs and several technical limitations are current obstacles to widespread use in clinical and investigational settings.
References
1. Covic A, Voroneanu L, Apetrii M, et al. PTH and/or bone histology: are we still waiting for a veredict from the CKD-MBD grand jury? Am J Kidney Dis. 2016;67(4):535-538. [ Links ]
2. Carvalho C, Alves CM, Frazão JM. The role of bone biopsy for the diagnosis of renal osteodystrophy: a short overview and future perspectives.J Nephrol. 2016;29(5):617-26. [ Links ]
3. Vervoloet MG, Brandenburg VM. Circulating markers of bone turnover. J Nephrol. 2017; doi: 10.1007/s40620-017-0408-8. [ Links ]
4. Evenepoel P, Cavalier E, D´Haese PC. Biomarkers predicting bone turnover in the setting of CKD. Curr Osteoporos Rep. 2017;15(3):178-186. [ Links ]
5. Tan SJ, Cai MM. Is there a role for newer biomarkers in chronic kidney disease-mineral and bone disorder management? Nephrology (Carlton). 2017;22(2):14-18. [ Links ]
6. Chiang C. The use of bone turnover markers in chronic kidney disease-mineral and bone disorders. Nephrology (Carlton). 2017;22(2):11-13. [ Links ]
7. Gal-Moscovici A, Sprague MS. Role of bone biopsy in stages 3 to 4 chronic kidney disease. Clin J Am Soc Nephrol. 2008;3(3):S170-S174. [ Links ]
8. Kidney Disease: Improving Global Outcomes (KDIGO) CKD_MBD Work group. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention and treatment of chronic kidney disease-mineral bone disorder (CKD-MBD). Kidney Int Suppl. 2009;113:S1-S130. [ Links ]
9. Ketteler M, Block GA, Evenepoel P, Fukagawa M, Herzog CA, McCann L, et al. Executive summary of the 2017 KDIGO Chronic Kidney Disease-Mineral andBone Disorder (CKDMBD) Guideline Update: whats changed and why it matters. Kidney Int. 2017;92(1):26-36. [ Links ]
10. Gardham C, Stevens PE, Delaney MP, LeRoux M, Coleman A, Lamb EJ. Variability of parathyroid hormone and other markers of bone mineral metabolism in patients receiving hemodialysis. Clin J Am Soc Nephrol. 2010;5(7):1261-1267. [ Links ]
11. Sprague SM, Bellorin-Front E, Jorgetti V, et al. Diagnostic accuracy of bone turnover markers and bone histology in patients with CKD treated by dialysis. Am J Kidney Dis. 2016;67(4):559-566. [ Links ]
12. Bervoets AR, Spasovski GB, Behets GJ, et al. Useful biochemical markers for diagnosing renal osteodystrophy in predialysis end-stage renal failure patients. Am J Kidney Dis. 2003;41(5):997-1007. [ Links ]
13. Lehmann G, Ott U, Kaemmerer D, Schuetze J, Wolf G. Bone histomorphometry and biochemical markers of bone turnover in patients with chronic kidney disease stages 3-5. Clin Nephrol. 2008;70(4):296-305. [ Links ]
14. Urena P, Hubry M, Ferreia A, Ang KS, de Vernejoul MC. Plasma total versus bone alkaline phosphate as markers of boné turnover in hemodialysis patients. J Am Soc Nephrol. 7(3):506-512. [ Links ]
15. Massy Z, Drueke T. Adynamic bone disease is a predominant pattern in early stages of chronic kidney disease. J Nephrol. 2017; doi: 10.1007/s40620-017-0397-7. [ Links ]
16. Drechsler C, Verdujin M, Pilz S, Krediet RT, Dekker FW, Waner C et al. Bone alkaline phosphatase and mortality in dialysis patients. Clin J Am Soc Nephrol. 6(7):1752-1759. [ Links ]
17. Behets GJ, Viaene L, Meijers B, Blocki F, Brandenburg VM, Verhulst A, et al. Circulating levels of sclerostin but not DKK1 associate with laboratory parameters of CKDMBD. PLoS One. 2017;12(5):e0176411. [ Links ]
18. Smith ER. The use of fibroblast growth factor 23 testing in patients with kidney disease. Clin J Am Soc Nephrol. 2014;9(7):1283-1303. [ Links ]
19. Sharma AK, Toussaint ND. Is there a practical role for a virtual bone biopsy using highresolution imaging of bone in patients with chronic kidney disease? Nephrology. 2017; 22(2):27-30. [ Links ]
20. Pullman JM, Coco M. Noninvasive image of bone microarchitecture in pateints receiving renal transplant: can it replace histology? Clin J Am Soc Nephrol. 2017;4(12):562-564. [ Links ]
21. Moorthi RN, Moe SM. Recent advances in the non-invasive diagnosis of renal osteodystrophy. Kidney Int. 2013;84(5):886-894. [ Links ]
22. Bover J, Bailone L, López-Báez V, Benito S, Ciceri P, Galassi A, et al. Osteoporosis, bone mineral density and CKD-MBD: treatment considerations. J Nephrol. 2017; doi: 10.1007/ s40620-017-0404-z. [ Links ]
23. Naylor K, Prior J, Garg A, Berger C, Langsetmo L, Adachi JD, et al. Trabecular bone score and incident fragility fracture risk in adults with reduced kidney function. Clin J Am Soc Nephrol. 2016;11(11):20132-2040. [ Links ]
24. Iiomori S, Mori Y, Akita W, et al. Diagnostic usefulness of bone mineral density and biochemical markers of bone turnover in predicting fracture in CKD stage 5D patients – a single-center cohort study. Nephrol Dial Transplant. 2012;27:345-351. [ Links ]
25. Parker CR, Freemont AJ, Blackwell PJ, Grainge MJ, Hosking DJ. Cross-sectional analysis of renal transplantation osteoporosis. J Bone Miner Res. 1999;14:1943-1951. [ Links ]
26. Coco M, Pullman J, Cohen HW, Lee S, Shapiro C, Solorzano C, et al. Effect of risedronate on bone in renal transplant recipients. J Am Soc Nephrol. 2012;23:1426-1437. [ Links ]
27. Naylor K, Prior J, Garg A, Berger C, Langsetmo L, Adachi JD, et al. Trabecular bone score and incident fragility fracture risk in adults with reduced kidney function. Clin J Am Soc Nephrol. 2016;11(11):20132-2040. [ Links ]
28. Luckman M, Hans D, Cortez N, Nishiyama KK, Agarawal S, Zhang C, et al. Spine trabecular bone score as an indicator of bone microarchitecture at the peripheral skeleton in kidney transplant recipients. Clin J Am Soc Nephrol. 2017;12(4):644-652. [ Links ]
29. Alexander AJ, Jahangir D, Lazarus M, Spraguet SM. Imaging in chronic kidney diseasemetabolic bone disorder. Semin Dial. 2017; doi: 10.1111/sdi.12598. [ Links ]
30. Torres A, Lorenzo V, Gonzalez-Posada JM. Comparison of histomorphometry and computerized tomography of the spine in quantitating trabecular bone in renal osteodystrophy. Nephrol. 1986;44(4):282-287. [ Links ]
31. Jamal SA, Gilbert J, Gordon C, Bauer DC. Cortical pQTC measures are associated with fractures in dialysis patients. J Bone Miner Res. 2006;21(4):543-548. [ Links ]
32. Pocock N. Use of dual energy X-ray absorptiometry, the trabecular bone score and quantitative computed tomography in the evaluation of chronic kidney disease-mineral and bone disorders. Nephrology. 2017; 22(2):19-21. [ Links ]
33. Wehrli WF, Gomberg BR, Saha PK, Song HK, Hwang SN, Snyder PJ, et al. Digital topological analysis in vivo magnetic resonance microimages of trabecular bone reveals structural implications of osteoporosis. J Bone Miner Res. 2001;16(8):1520-1531. [ Links ]
34. Folkesson J, Goldenstein J, Carballido-Gamio J, Kazakia G, Burghardt AJ, Rodriguez A, et al. Longitudinal evaluation of the effects of alendronate on MRI bone microarchitecture in postmenopausal osteopenic women. Bone. 2011;48(3):611-621. [ Links ]
35. Wherli FW, Leonard MB, Saha PK, Gomberg BR. Quantitative high-resolution magnetic resonance imaging reveals structural implications of renal osteodystrophy on trabecular and cortical bone. J Magn Reson Imaging. 2004;20(1):83-89. [ Links ]
36. Rajapakse CS, Bhagat YA, Sun W, Magland JF, Wehrli FW. Micro-MR imaging-based computational biomechanics demonstrates reduction in cortical and trabecular bone strenght after renal transplantation. Radiology. 2012;262(3):912-920. [ Links ]
37. Techawiboonwong A, Song HK, Leonard MB, Wehrli FW. Cortical bone water: in vivo quantification with ultrashort echo-time MR imaging. Radiology. 2008;248(3):824-833. [ Links ]
38. Link TM, Sabarowski, Kisters K, Kemphes M, Kosh M, Newitt D, et al. Changes in calcaneal trabecular bone structure assessed with high-resolution MR imaging in patients with kidney transplantation. Osteoporosis Int. 2002;13(2):119-129.
Carolina Lã Belino, MD
Nephrology Department; Centro Hospitalar Vila Nova de Gaia e
Espinho Rua Conceição Fernandes 4434 -502 Vila Nova de Gaia, Portugal
E -mail: carolinabelino@hotmail.com
ACKNOWLEDGMENTS
We thank Prof. Doctor João Frazão for all the knowledge, support and availability provided.
Disclosure of potential conflicts of interest: none declared
Received for publication: Nov 21, 2017
Accepted in revised form: Dec 21, 2017


{kind=link}