











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
Acute kidney injury (AKI) is common in neonates, children, and adolescents, particularly if critically ill and admitted to an intensive care unit. We currently know that AKI is an important factor for longterm prognosis in children and that these patients should be carefully monitored. However, AKI is still underdiagnosed in Pediatrics and these children are seldomly followed at a Pediatric Nephrology Clinic.
In this review we will mainly focus on how to prevent and promptly diagnose pediatric AKI.
DEFINITION AND CLASSIFICATION OF PEDIATRIC AKI
AKI is characterized by a sudden decrease in kidney function leading to the retention of nitrogenous waste products and acid-base and electrolytes imbalance.1,2
Several AKI classification systems have been developed throughout the years. In 2004, the Acute Dialysis Quality Initiative presented the Risk, Injury, Failure, Loss, End-Stage Renal Disease (RIFLE) criteria.3 Afterwards, the RIFLE criteria were adapted to the pediatric population Pediatric-modified RIFLE (pRIFLE). In 2007, the Acute Kidney Injury Network (AKIN) criteria were proposed.4,5Both pRIFLE and AKIN criteria were used in numerous studies involving children.6
In 2012, the Kidney Disease Improving Global Outcomes (KDIGO) criteria were developed, which are based on the combination of AKIN and RIFLE classifications. Nowadays, KDIGO criteria are the most used in pediatric AKI studies.
According to KDIGO, AKI is defined by the presence of one or more of the following:
• Rise in serum creatinine ≥ 0.3 mg/dL in 48 hours;
• Rise in serum creatinine ≥ 1.5 x the basal value of the past 7 days; or
• Urine output < 0.5 mL/kg/h in 6 hours.7
This definition has been validated for children and adults, excluding newborns.8 KDIGO defines three AKI severity stages, which are shown in Table 1. A higher stage translates to a higher risk of death and a higher need for kidney replacement therapy.9
Table 1 Acute kidney injury classification
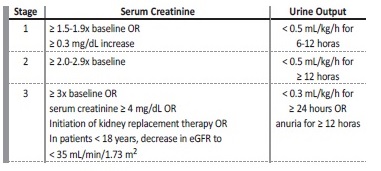
eGFR = estimated glomerular filtration rate
Adapted from: Kidney Disease Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. (2012). KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl. 2012; 2:138.7.
One-fifth of critically ill children with AKI have normal serum creatinine. In such patients, only a decrease in urine output is found.1 These children have a worse prognosis than those with AKI who only meet the serum creatinine criterion.1 Furthermore, children who meet both criteria have a worse prognosis than those who meet only one of them, having higher mortality rates, higher hospital lengths of stay and a higher risk of requiring kidney replacement therapy, invasive mechanical ventilation, and extracorporeal membrane oxygenation (ECMO). Therefore, both urine output and serum creatinine should be evaluated in each patient, to better identify children with AKI and to better recognize patients with potential worse prognosis.1,10
Informatics tools to immediately detect creatinine rises compatible with AKI should be implemented in every center in order to decrease AKI underdiagnosis.
LIMITATIONS OF THE CURRENT AKI DEFINITIONS AND STRATEGIES TO IMPROVE AKI EARLY DIAGNOSIS
KDIGO definition of AKI has several practical limitations since it involves knowing basal serum creatinine values and requires urine output monitoring.
First, blood tests are not required for the routine follow-up of a healthy child, so it is frequent not to have a basal serum creatinine available when evaluating a child in the emergency room. In order to overcome the lack of a baseline creatinine, several methods have been proposed, including back-calculating creatinine based on the Schwartz equation, full age spectrum (FAS), and CKiD-under-25 (U25) equations. Recently, a single-center retrospective analysis of pediatric patients (0-25 years) admitted from 2012 to 2019 was used to derive and validate a novel AKI baseline creatinine (ABC) estimation equation.11 This formula included only age and had a R2 = 59.9% and 73.2% of values within 30% of true baseline creatinine.11 The precision increased significantly when the equation included age and minimum creatinine within initial 72 hours (ABC-cr).11 The latter formula can more accurately estimate basal creatinine by ≥ 25% compared to previous methods.11 The potential applicability of these equations is immense, including earlier recognition of AKI and improved consistency of pediatric AKI definition.
Second, the urine output criterion included in KDIGO definition of AKI has low specificity since it may be influenced by factors such as hydration status or diuretic drug use. Oliguria can occur due to higher urine concentration without an actual decrease in kidney function.
On the other hand, diuretic drugs are some of the most used medications in the Intensive Care Units (ICUs), which can theoretically mask an AKI episode that would only be diagnosed using the urine output
criterion.12,13Furthermore, quantification of urine output is challenging in incontinent children without indwelling bladder catheters, which increase the risk of urinary tract infections.
More sensitive and specific biomarkers are needed for a better AKI diagnosis.7 It is well known that serum creatinine has low sensitivity, as levels tend to remain within normal ranges until approximately 50% of nephrons are lost or when the glomerular filtration rate (GFR) falls to 60 mL/min/1.73 m2.13 Therefore, serum creatinine is a late marker of decreased kidney function, with a rise in serum creatinine only occurring 2 to 3 days after the initial kidney insult.14,15Additionally, up to 15% of creatinine is secreted by tubules, which may lead to an overestimation of GFR and creatinine clearance. This overestimation is unpredictable and might vary in the same patient with declining GFR.13 In fact, when there is a decrease in GFR, tubular secretion of creatinine rises, and it may represent up to 50% of creatinine clearance.16 It should also be noticed that some drugs inhibit the tubular secretion of creatinine (such as trimethoprim), which might increase serum creatinine values, without real changes in kidney function.13
On the other hand, the production of creatinine from muscle catabolism might be negatively influenced by severe liver disease and positively influenced by rhabdomyolysis, making serum creatinine levels dependent on muscle mass.
Hydration status also changes serum creatinine levels, and fluid overload may dilute creatinine leading to falsely low levels of this marker.12,13,17
Recently, the renal angina index was developed, which helps predict the likelihood of developing AKI stage 2 or 3, three days after its evaluation, which should happen 12 hours after a patient is admitted to a Pediatric Intensive Care Unit (PICU). This index showed a better performance in predicting AKI than isolated increases in serum creatinine.18 AKI prediction allows an earlier implementation of nephroprotective measures.
It is important to distinguish the concepts of risk of AKI, kidney damage, AKI and kidney failure. Risk of AKI refers to the exposure to a risk factor that may directly trigger the kidney injury process and/or the existence of susceptibility factors that affect the prognosis after exposure to a triggering factor.7 Kidney damage refers to an intermediate stage between risk of AKI and AKI itself, in which there is subclinical pathology or other changes in kidney function other than a decrease in GFR. As previously mentioned, AKI is defined as a decrease in kidney function expressed as a reduction in GFR. Finally, kidney failure represents a stage of AKI in which GFR is less than 15 mL/min/1.73 m2 or in which kidney replacement therapy is required.
Serum creatinine rise is only observed when there is an established change in kidney function and a decrease in GFR.19 On this matter, other biomarkers which may allow AKI identification sooner in the course of the illness, or which may identify the stages of kidney damage and risk of AKI have been studied. These include the neutrophil gelatinase-associated lipocalin (NGAL), interleukin-18 (IL-18), kidney injury molecule-1 (KIM-1) and liver fatty acid binding protein (L-FABP).12,20,21
NGAL is the most studied novel biomarker, and it is already being used in clinical practice in many centers. Urinary NGAL levels rise when kidney tubules are damaged. In an NGAL reporter mouse model, prerenal AKI almost did not increase NGAL expression, while renal ischaemia elevated NGAL dramatically.22 This marker increased 6 hours after the insult and continued to be elevated until 24-48 hours after the insult.22 Moreover, NGAL levels correlated with the intensity of the insult, reflecting the damage caused to the kidney tubular epitelial cells.22 This biomarker is, therefore, particularly useful in rapidly identifying intrinsic renal AKI.22
In human studies it was also found that NGAL was increased in acute tubular necrosis and nephrotoxic induced injury, as well as post cardiopulmonary bypass AKI.2,23 Interestingly, in a prospective study, which included children and adolescents (aged between 1 month and 18 years old) admitted to a PICU, urinary NGAL levels were elevated (at least 6 times higher than controls) 2 days before there was a 50% rise in serum creatinine.24 Urinary NGAL is now being used in clinical practice to identify AKI earlier and to distinguish renal from prerenal AKI. This allows us to better identify the patients with worse prognosis who require more effective renoprotective measures and who may benefit from kidney replacement therapy. Urinary NGAL may be particularly useful in neonatal care, a setting where creatinine levels initially do not reflect the newborn GFR.
Furthermore, a 2022 systematic review and meta-analysis showed that urinary NGAL is an accurate biomarker for AKI in premature infants.25
Besides its function in the early identification of AKI episodes, these novel biomarkers might have a function in defining the prognosis. In a prospective study, which included children aged between 3 months and 14 years, NGAL levels were higher in patients with AKI that did not survive compared with those who survived. Moreover, NGAL levels were significantly higher in patients who required peritoneal dialysis and patients with higher NGAL levels had higher lengths of hospital stay.26
Furthermore, in another study it was found that children admitted to a PICU with both high urinary NGAL levels and high serum creatinine at admission had a higher risk of developing severe AKI by the third day of hospital stay compared with those who had a rise in sérum creatinine and normal urinary NGAL. Patients without a serum creatinine rise at admission, but with high levels of urinary NGAL had a higher risk of developing AKI by the third day of hospital stay, compared with those without a rise in urinary NGAL levels. Additionally, patients with high serum creatinine levels at admission but normal urinary NGAL levels were most likely to have brief and reversible forms of AKI.27
Taking into consideration the limitations regarding the use of sérum creatinine, such as its late rise in the course of AKI and how muscle mass and hydration status might change its levels, the simultaneous use of novel biomarkers, namely NGAL, might contribute not only to an earlier diagnosis, but also to the determination of prognosis, allowing a more personalized approach to these patients.27
Currently, a recommended approach to implement in the PICU setting will be the use of the combination of renal angina index and urinary NGAL, which showed sensitivity, specificity, and area under
the curve (AUC) of 0.76 (0.62-0.85), 0.89 (0.74-0.96), and 0.87 (0.84- 0.90) respectively for predicting severe AKI.28
EPIDEMIOLOGY OF PEDIATRIC AKI
AKI is common in critically ill children and adolescents, affecting one in four patients admitted to a PICU.18,29,30 Notably, AKI is the most frequent complication seen in critically ill children admitted to a PICU.31 AKI severity is associated with higher morbidity and mortality.18 These facts reinforce the need for AKI surveillance since admission.9
In the prospective study AWARE (Assessment of Worldwide Acute Kidney Injury, Renal Angina and Epidemiology in Critically Ill Children), conducted in 32 ICUs for 3 months and which included patients aged between 3 months and 25 years, without previous chronic kidney disease (CKD), the incidence of AKI was 26.9% (1261 in 4683 children).
The incidence of stage 2 AKI (moderate AKI) was 6.3% (294 in 4683 children) and of stage 3 AKI (severe AKI) was 5.3% (249 in 4683 children). In total, 1.5% of children (73 in 4683) required kidney replacement therapy. The 28-day mortality in patients with moderate and severe AKI was 11% (60 in 543 children), while it was only 2.5% (105 in 4140 children) in patients without moderate to severe AKI.9 This large prospective study clearly showed that AKI is common in critically ill children and adolescents and that it determines the prognosis.
AKI is also common in newborns admitted to Neonatal Intensive Care Units (NICUs). In the multicenter retrospective study AWAKEN (Assessment of Worldwide Acute Kidney Injury Epidemiology in Neonates) the incidence of AKI in newborns admitted to the NICU was 30%.10 The incidence was different according to gestational age: 48% in neonates born at 22-29 weeks; 18% in neonates born at 29-36 weeks; and 37% in neonates born after 36 weeks. In total, 1% (25 in 2022 newborns) required kidney replacement therapy, which represents 4% of all neonates with AKI (25 in 605 newborns). Neonates with AKI had higher mortality rates than neonates without AKI (10% of newborns with AKI vs 1% of newborns without AKI).10,32
In another study AKI occurred in 19.6% of the neonates.33 Caffeine administration before 29 weeks gestational age significantly decreased the incidence of neonatal AKI.33 The incidence of neonatal AKI was independently associated with death and extended length of hospital stay.33 Vancomycin, loop diuretics, intraventricular hemorrhage, surgical intervention, mechanical ventilation, and dopamine were independently associated with neonatal AKI.33
Notably, AKI plays a critical role in other organ development and injury, such as intraventricular hemorrhage and lung disease.34 Some preventive strategies for neonatal AKI have been suggested, including the use of caffeine in premature neonates, theophylline in newborns with hypoxic-ischemic encephalopathy, and reducing the use of nephrotoxic medication, as we will discuss further in this review.34
In a 2022 study, the overall rate of postoperative AKI among children undergoing noncardiac surgical procedures was 0.10%.35 Surgery times longer than 140 minutes, preexisting hematologic disorder, and preoperative sepsis were the strongest independent predictors of AKI.35
The 30-day mortality rate was higher in children who developed AKI (10.1% vs 0.19%; p < 0.001).35
Although frequent, AKI is underdiagnosed and referral to the pediatric nephrology clinic is scant.36,37 In a retrospective study, which included children and adolescents (aged between 1 month and 18 years), without previous CKD, seen in the pediatric emergency department (PED), AKI was identified in 1.5% (239 in 15 486). Only 19% of children and adolescents with AKI were diagnosed in the PED: these patients were older, had severe forms of AKI and were more likely to be admitted to the hospital.38 The most common causes of AKI were prerenal, followed by primary kidney disorders such as glomerulonephritis.38
In another retrospective study, which was performed at the Cincinnati Children’s Hospital Medical Center and included children and adolescents (aged less than 19 years), who were admitted to the hospital, AKI was identified in the first 48 hours in 10.4%. Stage 1 AKI represented 65.2%, stage 2 AKI 22.8% and stage 3 AKI 12.0%. Children with AKI were younger, were more likely to have had a past episode of AKI and had more previous hospital admissions. Moreover, history of solid organ transplant, congenital cardiac disease and receiving two or more nephrotoxic drugs were all associated with AKI development.
Out of all children with AKI, only 11.5% had the AKI diagnosis on their hospital discharge note.21
In a 2022, single center study AKI documentation, which was defined as any mention of AKI in the admission history and physical note, progress notes, or discharge summary, occurred in 34% (185/532) of AKI cases and 17% (90/532) had an inpatient pediatric nephrology consult.39 Among 501 survivors, 89 (18%) had AKI in their hospital discharge summary and 54 (11%) were followed at the Pediatric Nephrology clinic.39 Factors associated with AKI documentation were: stage 3 AKI, peak creatinine >1 mg/dL and longer length of stay. Stage 3 AKI and higher baseline creatinine were associated with inpatient pediatric nephrology consultation.39 Notably, inpatient pediatric nephrology consultation was positively associated with follow-up at the outpatient pediatric nephrology clinic, but documentation in the discharge summary was not.39 This study shows once again that the majority of AKI diagnoses were not documented and the proportion of children seen by a pediatric nephrologist was low.
In conclusion, AKI has a high incidence in several clinical settings, but it is still a largely underdiagnosed condition.
ETIOLOGY AND RISK FACTORS FOR PEDIATRIC AKI
AKI is a clinical syndrome with multiple possible etiologies. AKI is classically divided into prerenal, renal and postrenal categories, which represent respectively the pathophysiological mechanisms that lead to kidney hypoperfusion, structural kidney damage and urinary tract obstruction. The most common AKI etiologies in Pediatrics are the prerenal causes. These classification categories often include overlapping processes. For instance, in hypovolemic prerenal AKI the kidney hypoperfusion might be followed by acute tubular necrosis, and therefore renal AKI, as a result of a prolonged state of kidney hypoperfusion.40 The main causes of AKI in children are shown in Table 2.
Table 2 Acute kidney injury causes
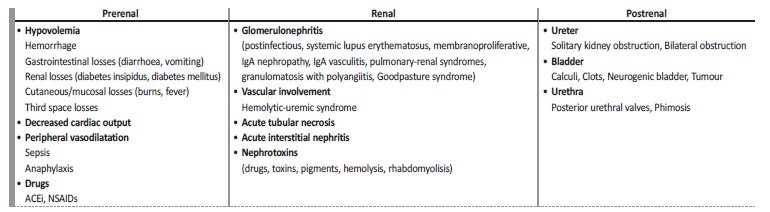
SIRS = systemic inflammatory response syndrome; ACEi = angiotensin-converting enzyme inhibitors; NSAIDs = non-steroidal anti-inflammatory drugs
Adapted from: Geary DF, Schaefer F, editores. Comprehensive pediatric nephrology. Philadelphia: Mosby/Elsevier; 200840; Whyte DA, et al. Acute renal failure in children. Pediatr Rev. 2008;29:299-306; quiz 306-7.57
In the past, the most common AKI etiologies in children included intrinsic kidney diseases, such as postinfectious glomerulonephritis, IgA vasculitis and hemolytic-uremic syndrome.6,41Nowadays, pediatric AKI often results from kidney hypoperfusion due to hypovolemia caused by dehydration or peripheral vasodilation in the context of sepsis. Other common etiologies include exposure to nephrotoxic medication and complications of other diseases which cause kidney hypoperfusion and/or direct kidney damage.6,21,41,42Some surgical procedures, namely cardiac surgery for congenital cardiac disease and solid organ and bone marrow transplantation, are also associated with a higher incidence of AKI.41 Exposure to nephrotoxic drugs has been increasing as a primary cause of AKI, accounting for 16% of AKI causes in children admitted to the hospital.42 The list of nephrotoxic drugs proposed in the Nephrotoxic Injury Negated by Just-in-time Action (NINJA) study is shown in Table 3.43
Table 3 List of nephrotoxic medications
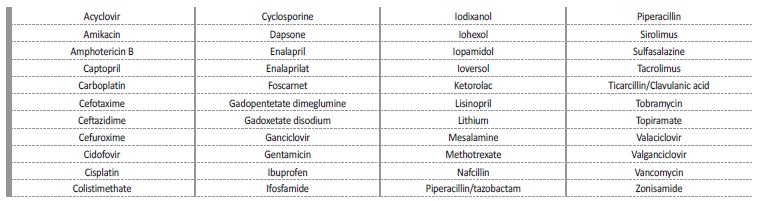
Adapted from: Goldstein SL, et al. Electronic Health Record Identification of Nephrotoxin Exposure and Associated Acute Kidney Injury. Pediatrics. 2013;132:e756-67.43
In a retrospective case-control study conducted in the Texas Children’s Hospital, which included children (aged less than 18 years) admitted to the hospital excluding those admitted to the PICU, found that 86% received at least one nephrotoxic drug.42 Furthermore, the percentage of patients who developed AKI increased with the rise in nephrotoxic drug exposure.42 Notably, younger children showed a higher risk of AKI development after nephrotoxic drug exposure.42 Taking this into account, identifying patients exposed to three or more nephrotoxic medications might be important for the early diagnosis and treatment of AKI.42
Treatment of newborns with nephrotoxic medications is also frequent, mainly among preterm neonates. In 2022, it was conducted a multicenter retrospective analysis of neonates admitted within the first two postnatal days, using the USA National Pediatric Hospital Information System Database. Treatment with 37 nephrotoxic medications was assessed.44 Of 192 229 neonates studied, 74% were treated with at least one nephrotoxic drug.44 Nephrotoxic medications were prescribed to 90%-95% of neonates born ≤ 28-week gestational age.44
Most treatments (95%-98%) occurred in the first 3 days.44 Aminoglycosides were the most frequent nephrotoxic drugs used; 28% of neonates were treated for ≥ 4 calendar days.44 Incidence of AKI was significantly higher in the treated group (aRR 3.68 [95% CI: 2.85, 4.75]).44 The long-term effects of nephrotoxic induced AKI in neonates on nephrogenesis will need to be further studied. Vancomycin is particularly nephrotoxic. The incidence of vancomycin associated AKI in children was found to be 11.8% (1.6%-27.2%).45
Risk factors that increased the likelihood of vancomycin associated AKI were identified as concomitant use of other nephrotoxic medications, increased trough concentrations, increased dose, longer duration of treatment, impaired renal function and if the patient required pediatric intensive care.45 In another study a maximum serum trough level of vancomycin above 24.35 μg/mL predicted vancomycin associated AKI.46
In the NINJA study, conducted at the Cincinnati Children’s Hospital Medical Center, a systematic electronic health record screening was implemented, based on an informatics alert after nephrotoxic drug exposure. Exposure was defined as receiving aminoglycoside for ≥ 3 days or ≥ 3 nephrotoxic drugs simultaneously. Daily sérum creatinine monitoring in exposed patients was performed and drug substitution was recommended to the physician taken care of the patient, if clinically possible (for example, replacing non steroidal anti inflammatory drugs with paracetamol or replacing vancomycin and aminoglycosides with less nephrotoxic antibiotics).43 A 3-year evaluation of this program showed a 38% decrease in nephrotoxic drug exposure and a 64% decrease in AKI incidence.47 This program clearly shows that it is possible to reduce AKI incidence in children and adolescents if we decrease the use of nephrotoxic drugs, which can sometimes be replaced by other less harmful drugs. This is a simple measure that should be implemented in every center, since it has an important clinical impact. For each patient we should use only the necessary nephrotoxic drugs and for the less amount of time possible. Combination of nephrotoxic drugs should be avoided, if clinically possible. If available, the serum levels of the nephrotoxic drugs should be measured and the doses adjusted. Furthermore, all doses of the drugs used should be adjusted according to the GFR.
All these simple measures really make a difference and significantly decrease AKI. The Pediatric community can promote these norms in clinical practice, which will definitely have a positive effect on the short and long-term prognosis of these children. In a 2022 study the potential healthcare cost savings from reduced CKD by preventing AKI with the NINJA program for a pediatric population through age 21 were assessed.48 The NINJA program was considered likely cost beneficial, with greater savings into adulthood by avoiding/delaying end-stage renal disease and its costs.48
PROGNOSIS OF PEDIATRIC AKI
AKI is associated with longer lengths of hospital stay, need for kidney replacement therapy and increased risk of death.18,20,21 Early AKI diagnosis is, therefore, essential to establish nephroprotective interventions, such as nephrotoxic drug use eviction; fluid overload prevention, aiming euvolemia and adequate kidney perfusion; and implementing other strategies to reduce morbidity and mortality, and improve the outcome.7,9,38
AKI is not a completely reversible phenomenon and long-term sequelae are seen in up to 70% of affected children.38 These sequelae include progression to CKD.14,38
In a study of children admitted to a PICU who were diagnosed with AKI only 57% (139 in 245 children) were alive after 3-5 years and 59% (17 in 29 children) had at least one sign of kidney injury (microalbuminuria, hyperfiltration or decreased GFR, hematuria and/or hypertension).41 However, only 35% of the children with signs of kidney injury were being followed by a pediatric nephrologist.41
In a prospective study of children who developed AKI at a PICU 10% (13 in 126) progressed to CKD in a 1-to-3-year period after the AKI episode. Furthermore, 47% (59 in 126) had a mild decrease in GFR (GFR 60-90 mL/min/1.73 m2), hypertension and/or hyperfiltration.6
In a retrospective study of children and adolescents (aged less than 18 years) admitted to a PICU, it was identified that even patients who had a stage 1 AKI episode had a significantly increased risk of CKD after a 5-year follow-up period.49
In a 2022 study on the long-term effects of neonatal AKI, including stage 1 AKI, office hypertension (systolic and/or diastolic BP ≥ 95th percentile), microalbuminuria (> 30 mg/g creatinine), and hyperfiltration (> 187 mL/min/1.73 m2) were present in 13.0%, 12.7%, and 9.7% of patients, respectively.50 Among the 27 patients who had a 24-hours ambulatory blood pressure monitoring, 16 (59.3%) had at least one sign of microalbuminuria, abnormal hypertension and/or non-dipping, or hyperfiltration.50 Even children who experienced stage 1 and 2 neonatal AKI are, therefore, at risk for subclinical kidney dysfunction.50
Even though we do not fully understand the underlying mechanisms of the progression from AKI to CKD, one of the pathophysiological pathways proposed includes endothelial dysfunction, tissue hypoxia and local inflammation with subsequent fibrosis.51,52Additionally, perivascular pericytes might play a part in AKI to CKD transition, as there is evidence showing pericytes differentiate into myofibroblasts in the context of kidney injury, contributing to the establishment of fibrosis.52 Wnt/β-catenin pathway is a critical regulator of kidney development that is up-regulated after injury and might also play a part in CKD progression through uncontrolled fibroblast activation and promotion of tubulointerstitial fibrosis.52 Tubular epithelial cell injury happening during AKI also plays a role in the perpetuation of inflammation and later fibrosis, as well as the production of proinflammatory cytokines such as IL-6, IL-1β and TNF-α.52
It is not fully known which patients are at the highest risk of developing CKD after an AKI episode. Certain AKI etiologies or disease severity might pose different risks.53 Therefore, after an AKI diagnosis, children should be periodically assessed to detect early signs of kidney dysfunction.41 Late referral to pediatric nephrology is linked with higher mortality and increased risk of dialysis dependence.38
KDIGO recommends patients should be evaluated 3 months after AKI to identify complete resolution, new onset CKD or worsening of pre-existing CKD.7 Vanmassenhove et al (2018) suggest an evaluation 3 weeks after an AKI episode, in patients with incomplete kidney function recovery.54 Dharnidharka et al (2020) postulate children should have a follow-up after an AKI episode, at least in stage 2 and stage 3 AKI cases.55
In children, higher kidney functional reserve might mask a kidney function decrease after an AKI episode during childhood, which might only become evident later in life.56 This emphasises the need for follow-up after an AKI episode.
CONCLUSION
AKI is common in Pediatrics, particularly in critically ill neonates, children and adolescents. Despite its high incidence, AKI is sill underdiagnosed. Several strategies to promote AKI early diagnosis should be implemented, including the use of informatics tools to rapidly identify AKI and novel urinary biomarkers, which can faster and more accurately detect AKI. Furthermore, the pediatricians have an important role in preventing AKI, by promoting euvolemia and reducing nephrotoxicity. Educational programs in the pediatric community are essential to increase awareness about AKI and promote a change in clinical practice that will decrease AKI incidence, improve its early detection, increase Pediatric Nephrology referrals and, most importantly, improve the prognosis of these children.

