










Serviços Personalizados
Journal

Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
 Citado por SciELO
Citado por SciELO Links relacionados
 Similares em
SciELO
Similares em
SciELO Compartilhar

 Permalink
PermalinkNascer e Crescer
versão impressa ISSN 0872-0754versão On-line ISSN 2183-9417
Nascer e Crescer vol.27 no.4 Porto dez. 2018
https://doi.org/10.25753/BirthGrowthMJ.v27.i4.12947
CASE REPORTS | CASOS CLÍNICOS
A rare case of pediatric volvulus caused by a persistent omphalomesenteric cyst
Um caso raro de volvo intestinal causado pela persistência de um quisto onfalomesentérico
Catarina ValpaçosI, Mariana CostaI, Suzana FigueiredoI, Ana Raquel SilvaII, Jorge Correia-PintoII, Angélica OsórioII
I Pediatrics Department, Hospital de Santa Luzia, Unidade Local de Saúde do Alto Minho. 4904-858 Viana do Castelo, Portugal. catarinavalpacos@gmail.com; marianammcosta@hotmail.com; suzfigueiredo@gmail.com
II Pediatric Surgery Department, Hospital de Braga. 4710-243 Braga, Portugal. araquelosilva@hotmail.com; jcp@ecsaude.uminho.pt; angelicosorio@gmail.com
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
A persistent omphalomesenteric duct is one possible cause of small-bowel volvulus, a rare cause of acute abdomen in children.
A four-year-old child was admitted to the Emergency Department with abdominal pain and incoercible vomiting, with neither abdominal guarding nor relevant abnormalities revealed in complementary diagnostic exams. Due to a significant clinical deterioration over a 48-hour observation period, the child was transferred to a tertiary hospital with pediatric surgery. An abdominal ultrasound revealing severe bowel distension and increased abdominal free fluid warranted an exploratory surgery, which identified a voluminous omphalomesenteric duct cyst.
When symptomatic, treatment of this condition is consensual and consists of surgical excision of the anatomical abnormality, either by laparoscopy or conventional surgery. The latter was performed.
Conclusion: A persistent omphalomesenteric duct is a rare condition that generally requires a high level of clinical suspicion for diagnosis to be made, being most commonly detected during surgery. Associated complications and mortality rates are high, and a timely intervention is key, since surgical removal is the only treatment option.
Keywords: Acute abdomen; Intestinal volvulus; Omphalomesenteric duct
RESUMO
A persistência do ducto onfalomesentérico pode ser responsável pela formação de um volvo intestinal na porção do intestino delgado, uma causa rara de abdómen agudo em crianças.
Uma criança de quatro anos de idade foi admitida no Serviço de Urgência por dor abdominal e vómitos incoercíveis, sem defesa abdominal nem alterações significativas nos exames auxiliares de diagnóstico. Devido a um agravamento clínico significativo no período de 48 horas em que esteve sob observação, foi transferida para um hospital terciário, com acesso a cirurgia pediátrica. Uma nova avaliação ecográfica abdominal, que demonstrou extensa distensão abdominal e presença de líquido livre, levou a exploração cirúrgica, tendo sido identificado e removido um volumoso quisto do canal onfalomesentérico.
Quando sintomática, a orientação terapêutica desta patologia é consensual, consistindo na excisão cirúrgica do defeito anatómico, que foi efetuada.
Conclusão: A persistência do ducto do canal onfalomesentérico é uma condição rara, cujo diagnóstico exige um elevado nível de suspeição, sendo muitas vezes detetado apenas durante a cirurgia. A taxa de complicações e mortalidade é elevada e uma intervenção atempada é essencial, dado que a remoção cirúrgica constitui a única opção de tratamento.
Palavras-chave: Abdómen agudo; Ducto onfalomesentérico; Volvo intestinal
Introduction
A small-bowel volvulus represents a surgical emergency due to the closed loop obstruction of this intestinal section.1 It may be caused by certain congenital conditions, such as malrotation of the midgut, a mesenteric cyst or, in very rare cases, a persistent omphalomesenteric duct (OMD). The OMD is described in 2% of children, with no gender preference but a much higher symptom incidence in males.2-4,6-8 Other related abnormalities have been described, such as umbilical hernia, intestinal atresia, small-bowel volvulus, exomphalos, cardiac malformations, and cleft lip/palate. An association with trisomies 13 and 21 has also been reported.9 It is a rare cause of acute abdomen of obstructive origin, with few cases described in the literature.10
Case report
A four-year-old girl (14 kg) with previous history of untreated constipation was admitted to the Emergency Department presenting with abdominal pain (initial onset four days prior to admission) and incoercible vomiting with an increasingly brownish content. At physical examination, the child was prostrated and pale, hemodynamically normal, with a diffusely painful abdomen but no muscle guarding. Complementary diagnostic exams at admission - blood tests, abdominal X-ray, and ultrasound - revealed no other abnormalities besides increased distension of bowel loops. Vomiting ceased after administration of ondansetron and a proton pump inhibitor, and the child remained hospitalized for clinical monitoring.
Exams were repeated twenty-four hours after admission due to progressive aggravation of the child’s condition. Leukocyte count was 15.520x109 (85.6% neutrophils) and C-reactive protein (CRP) was normal. An upright abdominal X-ray revealed abundant feces throughout the colon, but no noticeable air-fluid levels. No gas or stool emission was observed after rectal tube insertion. A computed tomography (CT) of the abdomen and pelvis was performed, which confirmed the colonic distension, with abundant rectal aqueous content and a small volume ascites on the right iliac fossa (RIF), but no fat densification or other signs of intra-abdominal infection.
Forty-eight hours after admission, the child’s condition worsened. She was tachycardic, febrile (although still hemodynamically stable), presenting with localized tenderness and a clear RIF guarding. A significant increase in leukocyte count (21.170x109, with neutrophil predominance - 87.7%) and 18.4 mg/dL CPR were observed. At this point, she was transferred to a tertiary hospital with pediatric surgery.
On admission, the child presented a widespread abdominal tenderness (significantly more intense in the RIF) and a hesitant gait with no claudication. Another abdominal ultrasound was performed, showing a clear increase in abdominal free fluid. A perforated appendicitis was suspected, and the child was subsequently subjected to an exploratory laparoscopy. During laparoscopic procedure, a tubular structure was detected, around which the small bowel was volvulated causing an important distension of the small bowel loops. Due to this extreme bowel distension and no possibility of increasing the pneumoperitoneum (child tolerated a maximum of 10 mmHg without ventilation compromise), an open laparotomy became the only feasible surgical option.
A voluminous omphalomesenteric duct cyst (4.2x3.1x2cm) was identified as causing the volvulation. The cyst was necrotic and perforated, and the peritoneal free fluid was purulent.
A derotation of the volvulus with excision of the channel and a bowel wedge resection at its point of origin were performed, followed by extensive peritoneal lavage. The histopathology of the surgical specimen revealed morphological features consistent with an omphalomesenteric cyst connected to an enteric segment with ischemic necrosis and festering.
The child had a good postoperative evolution, despite a surgical wound infection at day seven, which was successfully treated. Discharged ten days after surgery, she presented with a good general condition, required no diet restrictions, had a normal intestinal transit, and the surgical wound healing progressed favorably.
Discussion
The OMD is an embryonic structure that connects the yolk sac to the embryonic midgut during the first weeks of fetal development and is responsible for nutrient supply until the end of placental formation.4,10 This structure gradually becomes a thin fibrous band that, as from the fifth week of gestation (WG), starts to regress and is usually spontaneously absorbed by the seventh to tenth WG.3-5,9-10
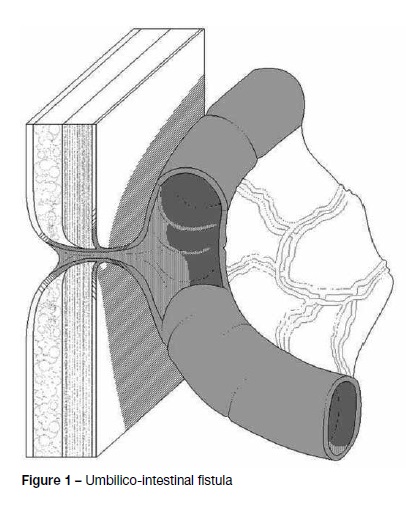
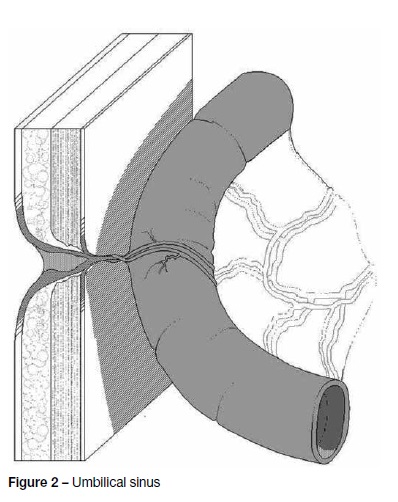
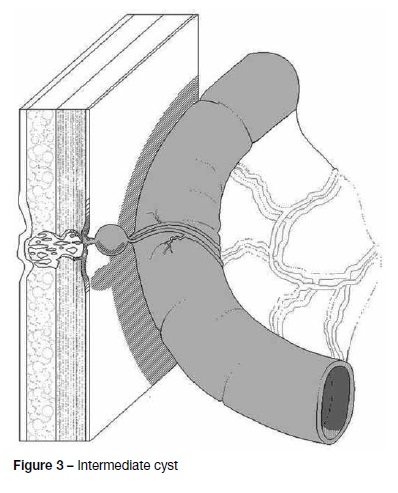
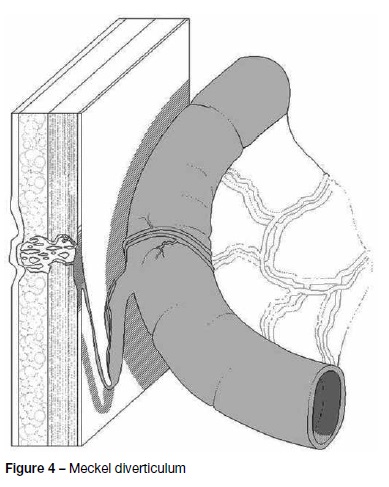
If a complete atrophy and disintegration of the OMD fails to occur, several anatomical abnormalities may arise. These may remain either open or closed, depending on whether the OMD remains pervious throughout its entire length or not.2-4,7 When an entirely open OMD persists, an umbilico-intestinal fistula develops (Figure 1). If the opening of the duct remains patent solely at its outer portion, an incomplete fistula results, which is known as umbilical sinus (Figure 2). In some cases, a mucous structure, closed at both ends, is formed along the fibrous cord, known as an intermediate cyst (Figure 3). The OMD may further persist as a sacculation or pouch connected to the ileum, known as Meckel diverticulum (Figure 4).2,5,8,10 This is the most common presentation of the embryonic structure.2-4,6-9
Persistence of OMD is observed in 2% of the population and may lead to complications in 20% of cases.4,8 Symptoms usually unfold before the age of four. In fact, in 73−85% of cases, symptoms occur during the neonatal period, when the presence of a fistula leads to pouring of fecal matter through the umbilicus, raising suspicion of this diagnosis.6,9-10 In these cases, the most serious complication is an acute mechanical obstruction of the small intestine.9 Intestinal occlusion may result from adhesions, volvulus, intussusception, or internal hernia, compromising normal function of bowel loops.7,10 Most often, it occurs by means of a volvulus around the remaining fibrous duct.8-9 Mortality occurs in nearly 18% of cases with severe complications.4
Diagnosis of such abnormalities can be established through an abdominal ultrasound or abdominal CT, or through a fistulography in cases of an open duct.6 Nevertheless, an intestinal obstruction diagnosis is not always easy and often only confirmed during surgical procedure.8
In this case report, persistence of OMD as a cyst, without an umbilical fistula, hindered its straightforward identification (Figure 3). The progressively severe abdominal pain, with obstipation and vomiting, raised the possibility of an intestinal occlusion from the beginning. However, absence of air-fluid levels on the x-ray and initial ultrasound and abdominal CT results postponed the surgical approach to when the child already presented with an acute abdomen. As pointed out in the literature, a high level of suspicion is required to intervene, namely in cases where imaging tests do not support the diagnosis (e.g. when interpretation is hindered by the interposition of large amounts of stool and gas across intestinal segments). In the present case, diagnosis was only confirmed during surgery, after identifying a structure responsible for an intestinal volvulus.
When symptomatic, treatment of this condition is unanimous and consists of surgical excision of the anatomical abnormality, either by laparoscopy or conventional surgery.3,9 A laparoscopic approach was initially attempted in this patient, but it revealed unsuccessful due to intestinal distension and preclusion of increasing pneumoperitoneum pressures. That would probably have been the best surgical option towards a more favorable postoperative recovery, with reduced pain and earlier discharge, lower probability of postoperative wound infection, and improved cosmesis.11
Opinions diverge on whether this is an incidental finding. While some argue that removal of the abnormality is not necessary in such cases, others emphasize the risk of serious complications, stating that surgical removal should always be performed.3,5-9.
A persistent OMD is a rare condition, generally requiring a high level of diagnostic suspicion and mostly detected during surgery. The rate of complications and mortality is high, and as surgical removal is the only treatment option, a timely intervention is essential.
REFERENCES
1. Vijayaraghavan SB, Ravikumar VR, Srimathy G. Whirlpool Sign in Small-Bowel Volvulus Due to a Mesenteric Cyst. J Ultrasound Med 2004; 23:1375-7. [ Links ]
2. Giacalone G, Vanrykel JP, Belva F, Aelvoet C, De Weer F, Van Eldere S. Surgical Treatment of Patent Omphalomesenteric Duct Presenting as Faecal Umbilical Discharge. Actachirbelg 2004; 104:211-3. [ Links ]
3. Ioannidis O, Paraskevas G, Kakoutis E, Kotronis A, Papadimitriou N, Chatzopoulos S, et al. Coexistence of Multiple Omphalomesenteric Duct Anomalies. Journal of the College of Physicians and Surgeons Pakistan 2012; 22:524-6. [ Links ]
4. Zafer Y, Yiğit Ş, Türken A, Tekinalp G. Patent Omphalomesenteric Duct. Turk J Med Sci 2000; 30:83-5.
5. Neyak B, Dash RR, Mallik BN. Multiple vitello-intestinal duct anomalies in a pediatric patient: A rare case report. Oncology, Gastroenterology and Hepatology Reports 2015; 4:30-1. [ Links ]
6. Mariño LP, Fraga JI, Rubio S, Segarra J, Gaetar M, Ossés JA. Persistencia del conductoonfalomesentérico. Arch Argent Pediatr 2009; 107:57-9. [ Links ]
7. Ccencho CG, Cydejko JCL, Aranguren CFG, Revoredo F, Tarazona AS, Ramírez VO. Persistencia de Conducto Onfalomesentérico como causa de Obstruccion Intestinal en el Adulto. Reporte de un caso en el Hospital Nacional Hipolito Unanue. Rev Gastroenterol Perú 2008; 28:154-7. [ Links ]
8. Herman M, Gryspeerdt S, Kerckhove D, Matthijs I, Lefere P. Small Bowel Obstruction due to a Persistent Omphalomesenteric Duct. JBR-BTR 2005; 88:175-7. [ Links ]
9. Mahato NK. Obliterated, fibrous omphalo-mesenteric duct in an adult without Meckel’s diverticulum or vitelline cyst. Romanian Journal of Morphology and Embryology 2010; 51:195-7.
10. Markogiannakis H, Theodorou D, Toutouzas KG, Drimousis P, Panoussopoulos SG, Katsaragakis S. Persistent omphalomesenteric duct causing small bowel obstruction in an adult. World J Gastroenterol 2007; 13:2258-60. [ Links ]
11. Blinman T, Ponsky T. Pediatric Minimally Invasive Surgery: Laparoscopy and Thoracoscopy in Infants and Children. Pediatrics 2012; 130:539-49. [ Links ]
Endereço para correspondência | Dirección para correspondencia | Correspondence
Catarina Valpaços
Pediatrics Department
Hospital de Santa Luzia
Unidade Local de Saúde do Alto Minho
Estrada de Santa Luzia 50
4904-858 Viana do Castelo
Email: catarinavalpacos@gmail.com
Received for publication: 23.08.2017
Accepted in revised form: 14.02.2018

