Serviços Personalizados
Journal

Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
 Citado por SciELO
Citado por SciELO Links relacionados
 Similares em
SciELO
Similares em
SciELO Compartilhar

 Permalink
PermalinkCadernos de Estudos Africanos
versão impressa ISSN 1645-3794
Cadernos de Estudos Africanos no.27 Lisboa jun. 2014
Its All About Sex: What urban Zimbabwean men know of labia minora elongation
Tem tudo a ver com sexo: O que os homens zimbabueanos sabem do alongamento dos pequenos lábios vaginais
Guillermo Martínez Pérez*, Concepción Tomás Aznar** e Harriet Namulondo***
*Departamento de Fisiatría y Enfermería, Facultad de Ciencias de la Salud, Universidad de Zaragoza, Calle Domingo Miral, s/n, 50009 Zaragoza, Espanha, gmartinezgabas@gmail.com
**Departamento de Fisiatría y Enfermería, Facultad de Ciencias de la Salud, Universidad de Zaragoza, Calle Domingo Miral, s/n, 50009 Zaragoza, Espanha, ctomas@unizar.es
***Departamento de Fisiatría y Enfermería, Facultad de Ciencias de la Salud, Universidad de Zaragoza, Calle Domingo Miral, s/n, 50009 Zaragoza, Espanha, hnamulondo2007@yahoo.com
ABSTRACT
Labia minora elongation is one of the vaginal practices that some Zimbabwean women engage in during the pre-menarche age. This practice has not been thoroughly investigated in Zimbabwe. The objective of this study is to learn about the knowledge, attitudes and perceptions of urban Zimbabwean men towards labia minora elongation. A qualitative study was conducted in Chitungwiza, Harare, in 2012. Thirty-one adult men were interviewed. Data was collected on mens understanding of the procedure, motivations, its relevance for marriage and sexual life, and its implications on health. The findings demonstrate that labia minora elongation is recognized in Zimbabwe as a practice that enhances the sexual pleasure for both male and female partners, and that there are no perceived harms to womens health. More research is necessary to better understand the role of labia minora elongation in sexuality and acceptance of HIV/STI barrier methods.
Keywords: labia minora elongation, female genital modifications, sexuality, vaginal practices, Zimbabwe
RESUMO
O alongamento dos pequenos lábios vaginais (labia minora) é praticado por algumas mulheres zimbabueanas antes de atingirem a fase menstrual. Esta prática não tem sido investigada em profundidade no Zimbábue. O objetivo deste estudo é analisar os conhecimentos, as atitudes e as perceções de homens zimbabueanos residentes em meios urbanos relativamente ao alongamento dos pequenos lábios. Esta análise tem por base um estudo qualitativo realizado em Chitungwiza, Harare, em 2012. Foram entrevistados 31 homens adultos. Foram recolhidos dados sobre a percepção dos homens acerca do procedimento, as motivações, a sua relevância para o casamento e para a vida sexual, e as suas implicações em termos de saúde. Os resultados mostram que o alongamento dos pequenos lábios é reconhecido no Zimbábue como uma prática que aumenta o prazer sexual para ambos os parceiros, e que não prejudica a saúde das mulheres. No entanto serão necessárias mais pesquisas para compreender melhor o papel do alongamento dos pequenos lábios na sexualidade e na aceitação de métodos de prevenção contra o HIV/DST.
Palavras-chave: alongamento dos pequenos lábios vaginais, modificações genitais na mulher, sexualidade, práticas vaginais, Zimbábue
Many women in sub-Saharan Africa practice a wide array of traditional body modifications and vaginal practices. The motivations to engage in vaginal practices are diverse and range from beautifying the genitals, improving hygiene and personal grooming, medicinal practices and health, and preparing for sexual intercourse. One of the vaginal practices that women engage in is labia minora elongation (hereafter LME). LME is common among women of some linguistic groups in easthern and southern Africa (Grassivaro Gallo & Villa, 2006; Martínez Pérez & Namulondo, 2011; Martínez Pérez, Tomás Aznar & Bagnol, 2013). This vaginal practice involves the manual stretching of the inner folds of the external genitalia, the labia minora, and sometimes the clitoris, often with the aid of certain oils, crèmes and utensils. Stretching is complete when the desired length, which usually ranges from 2 to 5 inches, is reached (Martínez Pérez, Tomás Aznar & Bagnol, 2013). Traditionally, young girls start elongating their labia before they reach menarche. Their paternal aunts, grandmothers or their female peers instruct them. The most commonly cited motivations reported by those who practice it are that it is a requisite for marriage, a socializing rite of passage that determines entrance into womanhood, and a physical feature that enhances sexual pleasure (Grassivaro Gallo & Villa, 2006; Koster & Price, 2008; Fusaschi, 2010, 2012; Martínez Pérez & Namulondo, 2011; Bagnol & Mariano, 2012; Martínez Pérez, Tomáz Aznar & Bagnol, 2013).
Within the last decade, authors from the fields of social science, psychology or anthropology have conducted research with the aim to learn how women perceive LME, how it is performed, and what are the motivations that drive its practice. Qualitative research has been conducted in Democratic Republic of Congo (Grassivaro Gallo, Mbuyi & Bertoletti, 2010), Lesotho (Khau, 2012), Malawi (Grassivaro Gallo, Moro & Manganoni, 2009; Pétursdóttir, 2010), Mozambique (Bagnol & Mariano, 2008, 2012), Rwanda (Koster & Price, 2008; Fusaschi, 2010, 2012), and Uganda (Grassivaro Gallo & Villa, 2006; Martínez Pérez & Namulondo, 2011). The risks and benefits for the health of women who practice LME are, however, still under-explored. Discomfort, irritation, swelling, edema and pain, have been described by some of the participants of the qualitative studies (Grassivaro Gallo & Villa, 2006; Fusaschi, 2010; Martínez Pérez & Namulondo, 2011; Martínez Pérez, Namulondo & Bagnol, 2013). Pain, irritation, itching, swelling and dyspaurenia related to LME were reported by 5% of 919 women who participated in a household based survey on vaginal practices that was carried out in Tete Province, Mozambique (Hull, Martin Hilber, Chersich, Bagnol, Prohmmo, Smit et al., 2011; Bagnol & Mariano, 2012). To our knowledge, this study from Tete is the only quantitative study conducted up to date that investigates the prevalence, frequency and associated health risks of LME.
No recent qualitative or quantitative data on LME prevalence, frequency, motivations or reported health risks exists for Zimbabwe. Williams (1969) and Gelfand (1973a, 1973b and 1979) documented some case reports of LME among female members of the Shona linguistic group. Aschwenden (1982) described LME as prevalent among the Karanga. These documents described the procedure and its cultural significance as one of the many components of the rites of passage to womanhood. As Williams (1969) explained almost half a century ago, after examining 124 female Shona presenting at the antenatal clinic with enlarged labia:
Labial elongation should serve normally to augment sexual compatibility and to promote marital stability, ever so precarious for humans. Undoubtedly it has also been exercised as an aid to fertility Flaccid enlarged lips also increase the potential control over intercourse for the defenseless woman. If she wishes to protect herself against intromission, the rolling up of the loose labia into the vagina effectively closes the os (Williams, 1969, p. 166).
More recently, in a joint report from UNICEF, UNFPA and IOM on gender-based violence in Zimbabwe, the authors document that LME is a common traditional practice in Mberengwa and Mudzi districts (Marsh et al., 2009). In this report, LME is included as a harmful traditional practice along with rape, lobola (bridewealth), denial of access to education, forced early marriage, wife inheritance, and prostitution. The report states that, according to some of the women that participated in the study, There is tremendous social pressure to conform to this practice (ibid., p. 38). In addition to this report, in a study carried out in the city of Norton, a peri-urban area 40 km West of Harare, LME is mentioned as a requisite for Chewa and Nyau girls to start chinamwari, the initiation rites period of seclusion (Thabethe, 2008). As in many other contexts where LME is practiced, this procedure is just one component of certain initiation rites which may contribute to how young girls construct their body image. LME is part of a sexual socialization process that takes place from birth (Mariano, 2007).
More studies exist, though, on other traditional vaginal practices, such as finger-cleansing, vaginal wiping, insertion of substances and consumption of aphrodisiacs. These practices are highly prevalent in Zimbabwe, even among women from urban areas (Ray, Gumbo & Mbizvo, 1996; Van de Wijgert, Mbizvo, Dube, Mwale, Nyamapfeni & Padian, 2001; Turner, Morrison, Munjoma, Moyo, Chipato & Van de Wijgert, 2010). Some of the herbs and substances employed by Zimbabwean women may serve to irritate and alter the integrity of the cervical and vaginal epithelium, leading to inflammation of the mucosa and disruption of the normal flora, thus eliminating the lactobacilli that form a barrier against colonization of STI pathogens and transmission of HIV (Van de Wijgert et al., 2001). It is also hypothesized that the use of these substances and practices is not compatible with HIV/STI barrier methods such as condoms, lubricants and topical vaginal microbicides (ibid., 2001; Turner et al., 2010; Martin Hilber, 2012; Bagnol & Mariano, 2012).
Male condoms might not be accepted by some Zimbabwean men since they prefer to engage in dry sex, and the spermicides and lubricants in condoms alter the characteristics – tightness, dryness and warmness – that women seek by engaging in vaginal practices (Civic & Wilson, 1996; Ray et al., 1996; Van de Wijgert et al., 2001; Turner et al., 2010; Bagnol & Mariano, 2012). There is no evidence on men refusing to use male condoms related to their expectations on their female partners having practiced LME. And no direct association between LME and HIV/STI transmission has been demonstrated (Martínez Pérez, Tomás Aznar & Bagnol, 2013). However, understanding LME and its role in sexuality and acceptance of barrier methods, can play a critical role in designing effective new HIV/AIDS prevention technologies and other health promotion strategies including the development of information, education and communication programs.
Purpose of this study
The main goal of this study is to learn what urban Zimbabwean men know of the LME procedure, what their attitudes towards LME are, and how they perceive it. Other objectives are to describe trends in the practice of the rite, explore its health risks and benefits, and understand its contribution to HIV/STI transmission.
No other study exists, to our knowledge, that investigates mens knowledge, attitude and perception of LME specifically carried out in Zimbabwe. This study reproduces the methodology previously used in a qualitative research conducted in Wakiso district, Uganda (Martínez Pérez & Namulondo, 2011). In Wakiso district, the male members of the Baganda linguistic group were assessed in order to determine the likelihood that they would be involved in health promotion interventions aiming at minimizing the impact of LME in the health of Baganda girls (Martínez Pérez & Namulondo, 2011).
Similar approaches in Egypt (Ragab, El-Mouelhy & Fahmy, 2012) support the need to understand mens knowledge, attitude and perception towards traditional practices. Men play a key role in influencing African womens engagement in traditional vaginal practices – including LME – which, ultimately, may harm their sexual and reproductive health to different extents (Martínez Pérez & Namulondo, 2011; Ragab et al., 2012).
Materials and method
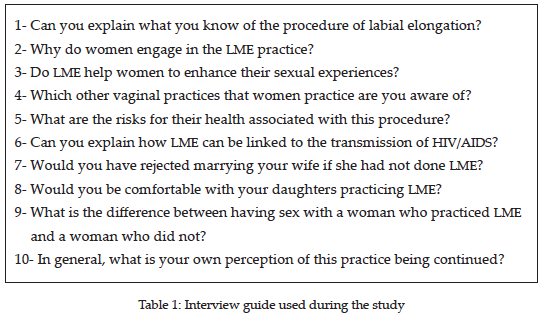
In this qualitative research, the semi-structured questionnaire used in the aforementioned study conducted in Wakiso district, Uganda, was adapted for this Zimbabwean setting (Martínez Pérez & Namulondo, 2011). Two questions were added about mens knowledge of other vaginal practices and of whether LME serves to enhance the sexual pleasure for the women (Table 1).
Chitungwiza, a high-density suburb 20 km southward of Harare was the study site. The respondents were purposively sampled, according to inclusion criteria, among the attendants to a local general practitioner´s clinic. The inclusion criteria for the respondents were being male, having ever engaged in heterosexual relationships, being above 18 years old, and, born and raised in Zimbabwe (regardless of linguistic group). All respondents that did not comply with these criteria were excluded from the study. The study was conducted between November 2012 and March 2013. Initially, local authorities were approached to receive permission for the interviews to be conducted, and the study protocol was reviewed and approved by the ethical review board Clinical Research Ethical Committee (IRB CEIC).
Standard ethical guidelines to protect the respondents anonymity and confidentiality were observed. The purpose of the study was explained to the respondents and they gave informed consent to participate in the study. No personal identifiers were requested from them. The respondents were aware they could withdraw from the study at any time and the data would then be destroyed ad hoc. Interviews were recorded. Once the interviews were transcribed and stored in a computer password-access protected, the recordings were erased.
Grounded theory was used as the methodological approach to analyze and code the data. Grounded theory requires purposeful sampling of individual cases from which data is then collected and analyzed from the beginning to recognize findings and simultaneously conceptualize those findings until saturation of data is reached (Sandoval Casilimas, 1996; Thabethe, 2008; Martin Hilber, 2012). Per grounded theory, the themes were identified out of the data itself, with no pre-existing hypothesis or expectations. The results were validated by triangulation with the information from the literature on LME in Zimbabwe (Williams, 1969; Gelfand, 1973a, 1973b, 1979; Aschwenden, 1982; Kanchense, 2007; Thabethe, 2008; Marsh et al., 2009) and with the information provided through key informant interviews with five female Zimbabweans key respondents from Chitungwiza who had knowledge on LME.
Results
Thirty-one respondents were enrolled in the study. All respondents were inhabitants of Chitungwiza and complied with the inclusion criteria. An overview of the demographics of the respondents are displayed in Table 2.
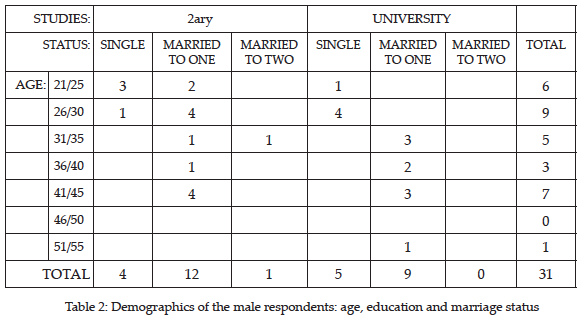
Fourteen of the respondents had completed university studies, while seventeen had completed secondary school. Twenty-one and one men were married to one and two women respectively. Nine were single in a relationship with at least one woman. With regards to their linguistic affiliation, twenty-eight had Shona as their mother tongue. Two and one respondents had Ndebele and Karanga as their mother tongue respectively. Fourteen respondents had fathered daughters. Twenty-eight respondents answered in English and three answered in Shona.
Knowledge on the procedure of labia minora elongation
According to all respondents, not all girls and women in Zimbabwe now practice LME. Young girls engage in LME before puberty or before the onset of the first menstruation. Women might start elongating at a later age if their male partners required it.
A girls aunt was mentioned as the most common person responsible for instructing the girls. The girls grandmothers, mothers, caregivers, sisters, and female peers and neighbors were identified as other instructors. The role of the paternal aunties as the one traditionally responsible to take the lead on the instruction on LME and other sexual matters was highlighted by some of the respondents:
Traditionally, in Shona culture, they learn it from the aunties, the sisters of the girl´s father. It is a tradition that is passed from generation to generation. It is part of the couching to the girls. Since there are other sensitivities involved, the girls do not shy away, they can disclose whatever they want to their aunts (Mike[1], 42 y.o., human resources administrator, married with two sons and two daughters).
LME is considered a womens secret, therefore young girls must hide away from mens sight to practice it. Girls practice LME indoors or in a private space such as their bedrooms. A few respondents said that girls might also practice in an outdoor space; such as kushinyamari, which is the special hut built for the celebration of the chinamwari or puberty initiation rites. LME is not a one-day process but requires significant investment of time. After the instructions, the girls continue practicing alone. Two men said that some girls might stretch in pairs, with other female peers assisting each other with the pulling.
The girls use their fingers to pull. The respondents described how the girls impregnate the labia minora with oils prepared with substances such as herbs, petroleum jelly, pfuta tree oil (castor bean tree), roast groundnuts, burnt bats wings, and with other unspecified traditional medicines that women obtain from traditional healers. One respondent mentioned the use of pliers to hold the vaginal lips and pull them out. The procedure of preparing the oils to aid the pulling was described by one respondent as follows:
They use some powder from a tree; pfuta. They start by roasting the seeds. Then they crash the seeds and get some powder and mix with Vaseline. Thats what they apply to start pulling (John, 33 y.o., teacher, married to two women, one son).Motivations behind the practice of LME
Enhancement of the sexual experience is the primary-cited purpose for engaging in LME. According to all respondents, women engage in LME with the aim to please their men, fulfill male expectations on the characteristics of their genitalia, arouse the men and increase mens sex drive:
Women do it for the men because it helps mens orgasm. The belief is that there is more sexual pleasure. For the (pleasure of) women I am not sure (Mike, 42 y.o., human resources administrator, married, two sons and two daughters).A common term that most respondents used to refer to the elongated labia is matinji. Matinji is not a derogatory term. On the contrary, the elongated labia or matinji are an appreciated physical feature. Some men described the matinji as toys or teddy bear for the men to play with during sexual foreplay[2]: The women do it to please their husbands. They say it (matinji) is their teddy bear. The husband needs something to play (John, 33 y.o., teacher, married to two women, one son).
Other reasons mentioned were that LME is a prerequisite for marriage, necessary for women to achieve womanhood and conform to culture. LME is considered to be useful in reducing pain during childbirth. A few respondents explained how some Zimbabwean women elongate their labia minora in order to persuade their partners to be faithful:
In terms of culture, because women live in a community where rumors say if you elongate men will not run away so therell be pressure to do it. Just a belief, a myth, a belief which is that if you enlarge your labia, the men tend to like you more (Alex, 42 y.o., human resources administrator, married, three daughters).One respondent explained how this practice could be analyzed from a psychoanalytical penis envy perspective:
Because for those labia elongated outside maybe they feel they have something tangible as well. Like the men have. That is the meaning of penis envy. She wants to have a penis. Penis envy, because if you ask the reason why they elongate it, most girls do not have a tangible reason (Daniel, 26 y.o., psychologist, married, one daughter).For twenty of the respondents, representing two thirds of the study sample, LME is perceived as a vaginal practice that contributes to enhanced female sexual experience. Only six men responded that women do not see their sexual pleasure enhanced with LME. To the majority, therefore, LME helps women to become sexually aroused during foreplay and to achieve orgasm during sexual intercourse:
They do enjoy it because the Shona women are sexually emotive. Women equally enjoy it as much as we (men) do and same as when we are fondling their breasts. Women get excited? Yeah! (Dhodho, 27 y.o., barber, married, one son and one daughter).Other vaginal practices
LME is the only vaginal practice of which one third of the respondents were aware. Secrecy around these traditional vaginal practices impeded Zimbabwean mens knowledge in this area. The vaginal practices other than LME that were mentioned by a few respondents were virginity tests, insertion of substances, herbs and wankie[3] to cause tightening of the vaginal canal, oral consumption of aphrodisiacs, and masuwo (lit. open the doorway) or insertion of herbs and medicines to enlarge the vaginal canal in preparation for delivery: When they are pregnant they do masuwo. This is how they prepare the way for the kid; they would be enlarging the vagina (Louis, 29 y.o., nurse, married, one son).
After losing virginity, women use medicines, black stones that they call wankie. They believe that after losing virginity the wankie can retain the virginity. Its like the contracting of the vagina (narrowing) so that men will believe they have found a virgin (Daniel, 26 y.o., psychologist, married, one daughter).A few men added that they themselves also ingest powders and herbal aphrodisiacs such as nmuti (lit. traditional herb, and also medicine) or vhuka vhuka (lit. wake up, wake up) for strengthening their backache or preventing loss of sexual drive or erectile dysfunction.
Implications for health
Half of the respondents identified a health implication for the girls and women that engage in LME.
Girls who refuse or fail to comply with LME, face the risk of stigma. This risk was explained by one respondent as follows:
If a woman does not yet have those large (labia minora) ones, she feels discomfort, even to bathe with women who have big ones. They extend for men to enjoy, to feel proud, because they consider that she is a true woman if she has extended those (labia minora) (Chris, 43 y.o., accountant, married, one son and two daughters).One respondent mentioned problems during labor derived from having elongated labia minora. A few respondents mentioned injuries, discomfort and cancer as a result of the use of the herbs. Discomfort was a symptom associated with the use of petroleum jelly, the labia folding and forming pockets of water inside the vagina, irritation if the labia were too elongated, and as consequence of the elongated labia getting in and out while walking. One respondent added that the women need to wear special pants to overcome the discomfort LME causes.
A third of the respondents highlighted an unexplained risk of infection. Two respondents believed that girls are at risk of acquiring bacterial infections when using public toilets:
If they go to a loo, sit in that seat, labia can come into contact with what; bacteria, infection. Then, someone with elongated labia has greater risk for taking infection than someone who is plain (Daniel, 26 y.o., psychologist, married, one daughter).For some men, there are perceived challenges of LME. One man explained that LME makes introduction of the penis difficult and that men have to be assisted by the women. Some respondents claimed that there is a risk of HIV/STI for men themselves. A few respondents explained that men are at risk of acquiring HIV/STI because women with elongated labia are promiscuous and might have many sexual partners:
Risk for the man because he may think they are virgins but they are not, they might be naughty. Those with long labia have many boyfriends. They are more promiscuous (Bill, 27 y.o., shopkeeper, single, no children).Most respondents did not establish any direct link on how LME could facilitate HIV/AIDS transmission. Four respondents explained that men prefer to feel and experience the elongated labia, hence refusing to wear a condom.
It must be discouraged because it can attract to unprotected sex Normally when you think of (sex) you are more focused on the sexual pleasure. But if someone is looking at the genital physical aspect, that person is more focused on unprotected sex. Because there is the belief that it can hold the men better and longer. They focus more on unprotected sex (Mike, 42 y.o., human resources administrator, married, two sons and two daughters).Other possible mechanisms of HIV/AIDS transmission were described. One respondent argued that HIV/AIDS transmission could happen in the presence of cuts in the labia minora. One other respondent said transmission might be the consequence of the use of pliers to assist with the stretching process. Another respondent explained that the risk of transmission is associated with the fact that women with elongated labia tend to lubricate more during sexual intercourse.
One respondent explained that the risk of HIV/AIDS transmission is actually for the men whose wives failed to elongate. According to this respondent, these men feel sexually unsatisfied and have to seek out other women with elongated labia with whom to have sex. Yes, there is a link. If a man is not satisfied because the woman did not do elongation that man will look for one with long labia, and that increases the risk for the man (Bruce, 45 y.o., driver, married, two sons).
Marriage prerequisite
None of the respondents said that either LME was a prerequisite for marriage for them or that they would have rejected their wives if they had not succeeded in practicing LME. Two respondents explained how they would not feel satisfied if their wives had not had elongated labia, and they seek sex with other women. However, to most respondents, men deciding to have extramarital affairs is not related to whether or not their wives had engaged in LME:
My wife did not do it. It is not important to me. But its true what women say that men want to pick other women. I personally do myself go with other women, you want to try that one and that other one (Eddi, 39 y.o., nurse, married, one son).Two men said that they would prefer to marry a woman that had not complied with LME. To these men, having LME is associated with women having more sexual drive: I prefer to marry one without. That one is more innocent (Bill, 27 y.o., shopkeeper, single, no children).
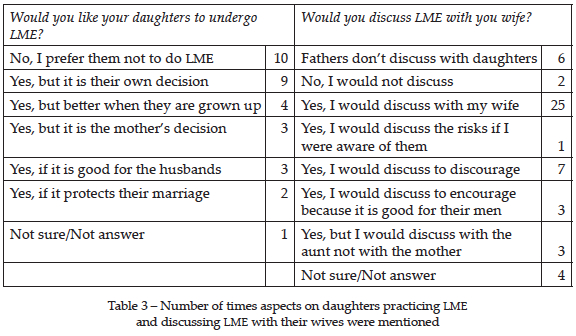
Attitude towards daughters
All interviewees – regardless of having fathered daughters or not – were asked if they would like their daughters to comply with LME (Table 3). A third of the respondents, ten men, stated that they would not want their daughters to practice it. Half of the respondents argued that the decision should be either the girls choice or the girl and her mother making the decision together. Four respondents clarified that they would prefer their daughters to decide to start LME once they were older and can make informed decisions to protect themselves:
I would not want my daughter to do it. I dont want to impose on her. I want it to be her choice so when she grows up a bit she can talk about it to her mother, and see if she decides it is good for her (James, 33 y.o., mechanic, married, one daughter).In a way I would like them to do it but when teenagers maybe they can go into promiscuity Id love if it was practiced better in their twenties. They are more mature then. Rather than when they are in their teens, in the school, being adolescents they maybe end up doing sex (John, 33 y.o., teacher, married to two women, one son).Three men said that they would encourage their daughters to engage in LME if their male partners required it. One respondent explained that having elongated labia guarantees that girls will get good, professional husbands. As two respondents explained, complying with LME is a bonding factor in marriage as it enhances the sexual experience for the male partner: Id prefer her not do it. But I would not discourage, because maybe she wants it to enjoy more sex with her husband (Edward, 28 y.o., doctor, single, one son).
The respondents were asked about the possibility of discussing LME with their female partners (Table 3). The majority of the respondents, twenty-five, said that they could talk openly to their wives about LME. Seven of these said that they would talk to their wives to ensure that their daughters do not undergo the practice. On the contrary, three said that they would talk to their wives to ensure that their daughters are elongating, since that is what men expect. One man said that he would talk to his partner if he were aware of any risks associated to labial elongation.
Only six men said they would not discuss LME with either their wives or their daughters. As for talking with their daughters directly, it was clear that fathers never talk to their daughters or even get to know if they are in the process of learning LME. One man said that he could not discuss it with his partner, but he could discuss with her aunt to ensure that the daughter is being instructed in LME. I would encourage because it protects their marriage. I would talk to my wife to encourage my daughters doing it (Barack, 30 y.o., barber, married, one son).
The importance of LME for sex
Five respondents explained that they had never had sex with a woman with elongated labia. According to seventeen of the respondents who had ever engaged in sexual intercourse with women who had complied with LME, there is no difference between having sex with women with or without elongated labia. To nine men, the sexual experience is more pleasurable with woman with elongated labia. However, only three respondents said that they preferred sex with a woman who did not practice LME. Some respondents argued that the preference for women with LME might be psychological. As one man pointed out:
Its all in the mind. I dont think there is any difference. Men try to cover up for their weaknesses in some areas probably loss of libido. Men need women to do this (LME). They say when she has not done that and they fail to perform, they say that the woman is the reason. Men blame the women. We usually as men dont accept the blame, we put it on women (Jim, 32 y.o., banker, married, two daughters).The men who said that they prefer sex with a woman that had complied with LME employed terms such as romantic, sweeter, beautiful, toys or teddy bear to describe the elongated labia.
Foreplay was described as crucial for half of the respondents. The elongated labia are enjoyed through fondling before intercourse. Foreplay arouses the men, boosts their sexual drive and helps women to reach orgasm. As some respondents explained:
There is a sensitivity that happens to you, when you are having intercourse the moment you insert your penis, it has got a swallowing effect. So women do it for the benefit of men, they want to get closer to a man, they do not want men to lose them, they just want to be the number-one girl type (Neil, 25 y.o., IT technician, single, no children).They think it (LME) stimulates the women to reach the orgasm. And the male call it toys for the husband. He can play with them (Barry, 22 y.o., student, single, no children).This matinji is great. It will wrap your penis, also that matinji if you dont have matinji you dont have a man. Men will be running away from you (Paul, 34 y.o., driver, married, two sons and one daughter).General perception
The respondents were asked to describe, in general, their opinion on LME being practiced in Zimbabwe. One third of the respondents, eleven men, felt LME should be discouraged:
Its just brainwashing each other. To get sex better. Some people who get matinji do not even get married. Others after having sex with a lot of people get divorced so there is no use. Some get married and they get divorced. So there is no use in matinjis. It is all about love. It should be discouraged. They should be educated about HIV rather than about pulling those matinjis (Phil, 29 y.o., cashier, married, one son).It is a waste of time. Men enjoy sex anyway with any woman. Men really do not mind. It better be discouraged in a way it promotes HIV because men do not want to use condom. Better to promote faithfulness (Edward, 28 y.o., doctor, single, one son).To a few respondents, instead of promoting LME, young girls should be taught how to accept the normal physical features they were born with:
As a Christian, I think the practice is like a sin. You are trying to do what the Bible forbids. You should stick to your normal features. Doing it is evil, why? It is based in to please men, while the Bible says you should pray, you should read the Bible. It should not be encouraged (Neil, 25 y.o., IT technician, single, no children).For another third of the respondents, ten men, LME should be promoted. Only a few respondents said that they did not have a clear stand on LME. According to some respondents, they would appreciate if more research be conducted on the health risks that are associated with LME:
More research should be done like a cohort analysis on this subject, just like theyre doing with circumcision so it can be known what are the benefits, risks, weaknesses. It might be a cultural practice that is not safe. Or it may be safe. So more research must be done so that my girls will be more informed (Daniel, 26 y.o., psychologist, married, one daughter).Discussion
The objective of this study was to learn how urban Zimbabwean men perceive the practice of LME, their knowledge of how LME is performed, and their attitudes towards this traditional practice. This paper has been titled Its all about sex because there was an overwhelming identification of LME by the respondents of this study as a cultural rite of which the main purpose is to enhance the sexual experience for both male and female partners.
LME is described as a practice that is kept secret by the women. However, the male respondents of this study are able to describe how the elongated labia minora, which they termed matinji, are achieved. The men also hold knowledge about the age at which the girls start elongating, who is responsible for instructing the girls, and even some of the herbs or substances that are employed to aid the pulling. The discussion held with the group of five female key informants from Chitungwiza was helpful to corroborate the accuracy of the information on the procedure of labial elongation that was provided by the male respondents. An area in which men lack knowledge, however, is around other vaginal practices in which their female partners might engage in. This is consistent with the findings of the literature and the female key respondents opinion; even if the decision to engage in vaginal cleansing, drying and tightening practices is made by the women to please their partners, the men are not expected to know what women do intravaginally (Van de Wijgert et al., 2001; Turner et al., 2010).
A common motivation that supports the practice of LME among certain linguistic groups in Zimbabwe is keeping male partners faithful (Thabethe, 2008). The participants of this study mentioned that some women engage in LME to prevent their male partners from seeking sexual experiences with other women. Nevertheless, from the narratives of the male respondents, it is not possible to conclude that men might be unfaithful if their female partners had not elongated their labia minora. In addition, the female key informants expressed that men are unfaithful regardless of their female partners genital appearance. Reasons, aside from lack of compliance with LME, which lead some men to seek sex outside marriage must be explored in future studies.
Chigidi (2009) describes how Shona elders inculcate taboos or avoidance rules in their children. The Shona educate their offspring to conform to their societal and cultural rules by means of lying to them or making them fear the consequences of failing to comply with the traditional norms and expectations (Gelfand, 1979; Chigidi, 2009). For future studies, it would be interesting to explore if promoters or instructors of LME intentionally use of lies and fears – e.g. not being able to keep a partner faithful, get married, or bear children – in order to have young girls comply with this traditional vaginal practice.
To the male respondents and the female key informants of this study, LME does not involve any major harm to the health of the women. On the contrary, as mentioned above, it is widely perceived as a cultural practice that benefits the sexual health of both partners because it aims to enhance the sexual experience. This is consistent with the findings of other qualitative studies on LME carried out in Malawi (Pétursdóttir, 2010), Mozambique (Bagnol & Mariano, 2012), Rwanda (Fusaschi, 2010) or Uganda (Martínez Pérez & Namulondo, 2011). However, this finding is inconsistent with other qualitative studies in which pain has been widely identified as a common adverse effect of LME (Grassivaro Gallo & Villa, 2006; Martínez Pérez & Namulondo, 2011; Martínez Pérez, Tomáz Aznar & Bagnol, 2013). No other symptoms, such as irritation, itching, swelling, and dyspaurenia, which are, together with pain, the most common adverse effects of LME reported by participants of the household survey in Tete, Mozambique (Hull et al., 2011; François, Bagnol, Chersich, Mbofana, Mariano, Nzwalo et al., 2012), were mentioned by either the male respondents or the female key informants of this study.
There is no evidence that LME may directly lead to an increased risk of HIV/AIDS transmission (Martínez Pérez, Tomás Aznar & Bagnol, 2013). In this study, practically none of the respondents established any direct link between LME and HIV/AIDS transmission. However, some of the themes that emerged in this study deserve a more thorough analysis, such as if, as some respondents discussed, the instructions that girls receive at the age when they start LME might mislead them to early sexual initiation and unprotected sex with multiple partners. Another aspect that deserves further attention is whether men or women might refuse to use male or female condoms and topical vaginal microbicides because these HIV/AIDS prevention technologies prevent them from obtaining what their expectations from sex dictate (Ray et al., 1996).
It should be further assessed, as well, if LME could be a decreasing trend in urban areas, especially among younger generations in Harare, Zimbabwe. Some of the findings from the male respondents of this study suggest that LME is becoming less prevalent in urban areas in Zimbabwe. They noted such beliefs, as the practice not being a prerequisite for marriage, many men not being willing to see their daughters being instructed in this tradition, and the majority of the respondents considering that there is no difference in sexual pleasure that related to whether or not their partners complied with LME.
Most of vaginal practices in which women engage, including LME, are reinforced by the motivation to satisfy their male partners preferences and expectations. However, secrecy around these practices impedes communication between men and women. Lack of communication means that men might not be knowledgeable about the implications for sexual health that may derive from some traditional practices, such as intravaginal insertion of certain corrosive substances. An important advocacy point is the promotion of discussion and information-sharing forums between men and women. In these forums, advice for alleviating the minor effects, such as pain and discomfort which are associated with the start of the practice of LME, can be discussed (Martínez Pérez & Namulondo, 2011). Moreover, mens acceptability can be assessed in terms of safer sex techniques and safer ways of performing vaginal practices that still hold the potential to satisfy their expectations of protection and pleasure (Ray et al., 1996). Comprehensive sex education targeting men can help to address the misunderstandings that men hold around traditional genital practices and their role in female health, sexuality and marriage (Ragab et al., 2012).
Study limitations and other future prospects
Data saturation in this study was achieved very early, and having enlarged the number of respondents would not have added much additional qualitative information. No significant differences were found regarding the socio-demographic variables collected. A more specific exploration into male and female traditional genital practices and its health implications must be achieved by implementing quantitative studies using questionnaires that can incorporate items to explore some of the themes emerged from this study and from previous research that have been published elsewhere (Ray et al., 1996; Van de Wijgert et al., 2001; Turner et al., 2010).
What this study failed to investigate is how men also attempt to increase their sexual performance or master their sexual prowess by making incisions or scarifications in their coccyx area, taking herbs valued as aphrodisiacs, or traditional foods such as mazondo or cows or pigs hooves, or applying Vicks and other concoctions in their penis (Aschwenden, 1982; Ray et al., 1996; Tsiko, 2010). This is another field that relates to notions of male sexuality and masculinity that this study did not explore in depth and that deserve further consideration.
Marsh et al. (2009) state that Zimbabwean women endure forms of gender-based violence throughout their life; rape and sexual exploitation, denial of access to education, emotional, physical and sexual abuse between intimate partners, forced early marriage, forced wife inheritance, and elongation of the labia minora. The narratives of the respondents of this study, in considering LME as a practice that might enhance the sexual experience for some men and women, do not sustain Kanchense (2007), Thabethe (2008) and Marsh et al. (2009) consideration of LME as a harmful practice in Zimbabwe of the same magnitude as other forms of gender based violence. More research is necessary, however, to determine how consistent with the hypothesis of Marsh et al. (2009) – and some of the respondents of this study – is the belief that having the young female disciplined in molding their genitalia to satisfy their male partners is a factor that favors HIV/STI transmission. The suggestion is that since the sexual instructions are believed by some to encourage girls to seek for sex at an age when they cannot make informed decisions on barrier methods use, it may increase this risk.
Conclusion
A qualitative study was conducted in Chitungwiza, a high-density dwelling southwards of Harare, Zimbabwe, aiming to learn on the knowledge, attitudes and perceptions of urban men towards LME. Thirty-one men participated in the study. LME is a cultural practice appreciated because it is thought to enhance the sexual experience for both male and female partners.
Common reasons reported in other settings, such as the rite being a requisite for marriage and for conception, were underreported by the study sample. The majority of men did not report any major implication for the health, neither positive nor negative, that is associated with LME. Men can be included in health promotion interventions aiming at discussing traditional practices with men and women. More research is necessary to understand how LME and other practices may promote the transmission of HIV/STIs or how it can inhibit men and women from using barrier methods such as condoms or topical vaginal microbicides.
References
Aschwenden, H. (1982). Symbols of life. Gweru, Zimbabwe: Mambo Press. [ Links ]
Bagnol, B., & Mariano, E. (2008). Elongation of the labia minora and use of vaginal products to enhance eroticism: Can these practices be considered FGM? Finnish Journal of Ethnicity and Migration, 3 (2), 42-53. [ Links ]
Bagnol, B., & Mariano, E. (2012). Gender, sexuality and vaginal practices. Maputo: Depar-tamento de Arqueologia e Antropologia, Faculdade de Letras e Ciências Sociais, Universidade Eduardo Mondlane. [ Links ]
Civic, D., & Wilson, D. (1996). Dry sex in Zimbabwe and implications for condom use. Social Science and Medicine, 42 (1), 91-98. [ Links ]
Chigidi, W. L. (2009). Shona taboos: The language of manufacturing fears for sustainable development. The Journal of Pan African Studies, 3 (1), 174-188. [ Links ]
François, I., Bagnol, B., Chersich, M., Mbofana, F., Mariano, E., Nzwalo, H., Kenter, E., Tumwesigye, N. M., Hull, T., & Hulber, A. M. (2012). Prevalence and motivations of vaginal practices in Tete Province, Mozambique. International Journal of Sexual Health, 24 (3), 205-217. [ Links ]
Fusaschi, M. (2010). Istituire il genere: Dominazioni e grammatiche della corporeità femminile in Rwanda. Voci, 1-2, pp. 159-171. [ Links ]
Fusaschi, M. (2012). Plaisirs croisés: Gukuna kunyaza. Missions, corps et sexualités dans le Rwanda contemporain. Genre, Sexualité & Societé, 8. In http://gss.revues.org/2571 [ Links ]
Gelfand, M. (1973a). Gross enlargement of the labia minora in an African female. Central African Journal of Medicine, 19 (5), 101. [ Links ]
Gelfand, M. (1973b). The genuine Shona. Survival values of an African culture. Gweru, Zimbabwe: Mambo Press. [ Links ]
Gelfand, M. (1979). Growing up in Shona society from birth to marriage. Gweru, Zimbabwe: Mambo Press. [ Links ]
Grassivaro Gallo, P., & Villa, E. (2006). Ritual labia minora elongation among the Baganda women of Uganda. Psychopathologie Africaine, 33, pp. 213-236. [ Links ]
Grassivaro Gallo, P., Moro, D., & Manganoni, M. (2009). Female genital modifications in Malawi: Culture, health and sexuality. In Denniston G. C., Hodges, F. M., & Milos, M. F. (Eds.), Circumcision and human rights (pp. 83-95). New York: Springer. [ Links ]
Grassivaro Gallo, P., Mbuyi, N. T., & Bertoletti, A. (2010). Stretching of the labia minora and other expansive interventions of female genitals in the Democratic Republic of the Congo (DRC). In Denniston, G. C., Hodges, F. M., & Milos, M. F. (Eds.), Genital autonomy: Protecting personal choice (pp. 111-124). Netherlands: Springer. [ Links ]
Hull, T., Martin Hilber, A., Chersich, M. F., Bagnol, B., Prohmmo, A., Smit, J. A., et al. (2011). Prevalence, motivations, and adverse effects of vaginal practices in Africa and Asia: Findings of a multicountry household survey. Journal of Womens Health, 20 (7), 1097-1109. [ Links ]
Kanchense, J. H. M. (2007). Urologic and gynecologic health problems among Zimbabwean women: What is the role of poverty? Urologic Nursing, 27 (5), 373-389. [ Links ]
Khau, M. (2012). Female sexual pleasure and autonomy: What has inner labia elongation got to do with it. Sexualities, 15 (7), 763-777. [ Links ]
Koster, M., & Price, L. L. (2008). Rwandan female genital modification: Elongation of the labia minora and the use of local botanical species. Culture, Health & Sexuality, 10 (2) 191-204. [ Links ]
Mariano, E. (2007). Projecto-piloto de diálogo entre medicina tradicional e convencional - Para uma prevenção do HIV/SIDA culturalmente sensível. Relatório de Pesquisa SUL (Govuro, Matutuine, Moamba, Magude). Maputo: CVM-MONASO-UEM. [ Links ]
Marsh, M., Kenny, E., & Jennifer, J. (2009). Joint UNICEF, UNFPA & IOM gender-based violence field mission Zimbabwe: May 2009. Harare, Zimbabwe: UNICEF. [ Links ]
Martin Hilber, A. (2012). Womens health, hygiene and HIV in Sub-Saharan Africa: The role of vaginal practices. PhD Dissertation. Faculty of Medicine and Health Sciences, Ghent University, Belgium. [ Links ]
Martínez Pérez, G., & Namulondo, H. (2011). Elongation of labia minora in Uganda: Including Baganda men in a risk reduction education program. Culture, Health & Sexuality, 13 (1), 45-57. [ Links ]
Martínez Pérez, G., Tomás Aznar, C., & Bagnol, B. (2013). Labia minora elongation and its implications on the health of women: A systematic review. International Journal of Sexual Health (published ahead of print). DOI: 10.1080/19317611.2013.851139 [ Links ]
Pétursdóttir, I. D. (2010). If I had a spear, I would kill the HIV beast: Views of a Malawi village on the HIV epidemics. Master Dissertation. Reykjavik, Iceland: Háskóli Íslands. [ Links ]
Ragab, A. R., El-Mouelthy, M. T., & Fahmy, A. (2012, September). Sexuality aspects of female genital mutilation: Mens perspectives. Conference Sexual Health and Rights in Africa, Windhoek, Namibia. [ Links ]
Ray, S., Gumbo, N., & Mbizvo, M. (1996). Local voices: What some Harare men say about preparation for sex. Reproductive Health Matters, 7, pp. 34-45. [ Links ]
Sandoval Casilimas, C. A. (1996). Investigación cualitativa. Bogotá: Instituto Colombiano para el Fomento de la Educación Superior. [ Links ]
Thabethe, S. N. (2008). A case of culture gone awry: An investigation on female initiation ceremonies and Nyau dance vigils on the rights of teenage girls to education and sexual reproductive health amongst migrant communities in Norton, Zimbabwe. Master Dissertation. Harare, Zimbabwe: University of Zimbabwe. [ Links ]
Tsiko, S. (2010). Amanqina Mazondo. Zimtravel, October, pp. 10-13. [ Links ]
Turner, A. N., Morrison, C. H., Munjoma, M. W., Moyo, P., Chipato, T., & Van de Wijgert, J. (2010). Vaginal practices of HIV-negative Zimbabwean women. Infectious Diseases in Obstetrics and Gynecology, 2010, 1-7. [ Links ]
Van de Wijgert, J., Mbizvo, M., Dube, S., Mwale, M., Nyamapfeni, P., & Padian, N. (2001). Intravaginal practices in Zimbabwe: Which women engage in them and why? Culture, Health & Sexuality, 3 (2), 133-148. [ Links ]
Williams, J. (1969). Labial elongation in the Shona. Central African Journal of Medicine, 15 (7), 165-166. [ Links ]
WHO (World Health Organization). (1996). FGM. Report of the WHO technical working group. July 17th-19th 1995. Geneva: WHO. [ Links ]
WHO (World Health Organization). (2008). Eliminating female genital mutilation. An interagency statement OHCHR, UNAIDS, UNDP, UNECA, UNESCO, UNFPA, UNHCR, UNICEF, UNIFEM, WHO. Geneva: WHO. [ Links ]
Recebido 1 de abril de 2013; Aceite 5 de março de 2014
Notes
[1] The respondents names quoted within the text do not correspond with their real names. Neither real names nor other personal identifiers were collected during the study.
[2] Matinji is a term that is also used in Tete province, central Mozambique. Similar metaphors comparing elongated labia with toys were also used by some of the male respondents of the study in Tete conducted by Bagnol & Mariano (2012).
[3] Van de Wijgert et al. (2001) describe wankie as ever been inserted intravaginally by 6% of a sample of 169 women in Harare. Wankie is described as a stone or sediment from Wankie (former name of nowadays Hwange District), which is pulverized or broken into small pieces and inserted inside the vagina in preparation for sexual intercourse.