










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkMotricidade
versão impressa ISSN 1646-107X
Motri. vol.15 no.1 Ribeira de Pena mar. 2019
https://doi.org/10.6063/motricidade14951
ARTIGOS ORIGINAIS
Motor Learning Process of Virtual Reality Tasks with Different Demands in Post Stroke Individuals
Giovanna C. Jangarelli1, Natalia A. Mazzini1, Murilo G. Almeida1, Tatiana B. Freitas1[*], Camila Torriani-Pasin1
1University of São Paulo, São Paulo -SP
ABSTRACT
Practicing tasks in Virtual Reality (VR) environment has shown to be effective for gain in cognitive and motor functions in post stroke individuals. However, there are few information about how the motor learning process of tasks with different demands occurs in this population, and if there are differences when compared with healthy individuals. The aim of the present study was to investigate the motor learning process of eight VR’s tasks with different cognitive and motor demands, in post stroke individuals (Experimental Group-EG), and compare it with healthy individuals (Control Group-CG). Eighteen individuals participated in the study performing eight sessions of practice, four for each task. The study involved: pre-test (1 session), acquisition phase (4 sessions for each task), post-test (1 session), and retention test (1 session after thirty days since the end of acquisition phase). The statistical analysis was run by a 2 x 3 ANOVA (groups x learning tests) with Tukey post hoc. At the end, EG group was able to learn three tasks, while CG learned four, one more than the ones learned by the post-stroke individuals. Task’s complexity affected, in more intensely the motor learning process in post-stroke individuals that with eight sessions were able to learn only low-complexity tasks.
Keywords: stroke, motor learning, virtual reality.
INTRODUCTION
Stroke effects in an individual may include motor and cognitive deficits, which can affect the motor learning process of a new motor skill and tasks (Boyd et al., 2009; Boyd & Winstein, 2004; Torriani-Pasin, 2010). The motor learning process can be defined as a modification in an individual’s proficiency of performance motor skills, by its relative long-lasting development (Magill, 2011).
That has been investigated since 2001, when Boyd and Winstein (2001) shown that the learning process of a sequence task was only able, in this population, with a previous knowledge of the sequence about to be practiced.
Since then, studies about motor learning process after a stroke has been done, and until the present moment, it is known that post stroke individuals have a slower velocity of learning new motor skills, when compared with healthy individuals (Boyd, Quaney, Pohl, & Winstein, 2007; Ioffe, Chernikova, Umarova, Katsuba, & Kulikov, 2010). In addition, their motor learning curves are similar to the one’s of healthy population, however it occurs latter (Bonuzzi et al., 2016; Boyd et al., 2007; Torriani-Pasin, Palma, & Freitas, 2016), needing more quantity of practice to achieve similar performance (Cirstea, Ptito, & Levin, 2006). Besides that, the corrections needed during the performance of a movement are also impaired (Platz, Denzler, Kaden, & Mauritz, 1994; Torriani-Pasin, Bonuzzi, Palma, Freudenheim, & Corrêa, 2018). Despite that, the acquisition and improvement processes of motor skills have been shown to be possible in post stroke population (Boyd et al., 2007; Cirstea et al., 2006; Platz et al., 1994). This have been stimulating an increase in the quantity of studies that investigate those processes and the factors that affect motor learning in these individuals (Adkins, Boychuk, Remple, & Kleim, 2006; Boyd et al., 2007; Ioffe et al., 2010; Kitago & Krakauer, 2013; Platz et al., 1994).
It is known that experience and practice are determinant factors of the motor learning process (Eerdt et al., 2010; Torriani-Pasin et al., 2018) as well as the environment where this occurs. Recently one of the options that has been widely used for post stroke population is the VR environment (Aminov, Rogers, Middleton, Caeyenberghs, & Wilson, 2018; Cho, Lee, & Song, 2012; Holden, 2005). Besides being motivating, it can stimulate cognitive and motor functions with a safe (Palma, 2016) progressive increase of task complexity levels (Mendes et al., 2012).
According to Pompeu et al (2014) the VR environment can offer a vast quantity of auditory and visual stimulus that can be used as external clues, an enormous quantity of attempts that can promote automation, and stimulate cognitive functions to solve different types of problems.
Although it has been well established in the literature the benefits of the VR environment, such as offering parameter control (da Silva Cameirão, Badia, Duarte, & Verschure, 2011; Laver, George, Thomas, Deutsch, & Crotty, 2015), security (Laver et al., 2017) and external focus of attention (Pompeu et al., 2014), but it is not known how the motor learning process of tasks in this environment occurs in post stroke individuals.
Bonuzzi et al (2016) has shown that, when it comes to a postural control task, in VR environment, both healthy and post stroke individuals are able to learn it, although the first ones were able to achieve higher levels of complexity. Similar results were obtained in Palma (2016), as post stroke group, after practicing a task that involved the displacement of the center of pressure, with different number of elements and processing load required, was capable to learn only the low-complexity task. One of the hypotheses is that cognitive deficits related to the planning and sequencing actions may have affected the motor learning process of higher complexity tasks in this population.
The aim of this study is to investigate the motor learning process of eight VR tasks with different motor and cognitive demands and complexities, after a stroke and compare it with healthy individuals.
METHOD
The present study is an experimental study that was approved by the Ethics in Research Committee of the School of Physical Education and Sport, of the University of São Paulo (CAAE: 40688114.9.0000.5391).
Participants
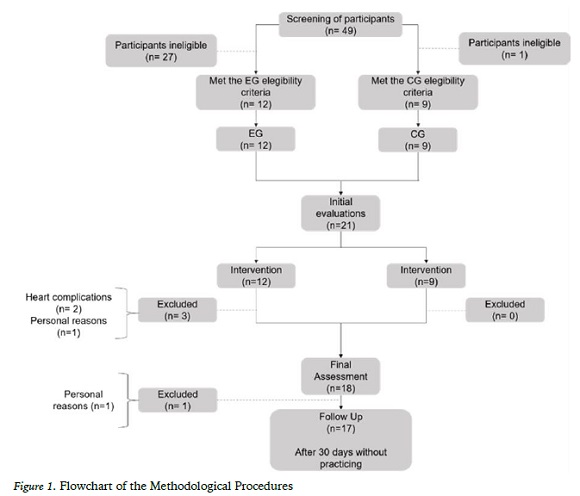
The sample was composed by eighteen individuals, being nine post-stroke individuals for the Experimental Group (EG), while nine healthy individuals for Control Group (CG). All of the participants or their legal persons read and signed the Informed Consent Form.
The inclusion criteria for the EG was: post stroke individuals with a single lesion of at least six months in anterior circulation territory, with at least 2 months without practicing any structured intervention, score higher than 24 at the Mini-mental State Examination (MMSE) (Bertolucci, Brucki, Campacci, & Juliano, 1994). Also, they could not have previous experience with VR.
The CG was composed by individuals paired by age and gender with the EG ones, without previous experience with STAbility And Balance Learning Environment (STABLE), without neurological or orthopedic diseases detectable by questioning at the time of the initial interview; with normal or corrected visual acuity and good auditory acuity (clinically evaluated); minimum of three years of schooling; and capable to come to the Motor Behavior Laboratory, at the School of Physical Education and Sport of University of São Paulo once a week to practice the tasks in VR’s environment. Individuals with cardiovascular complications that did not allow the physical exercise prescription and individuals that use drugs to reduce spasticity in at least six months were excluded from the study.
Measures
The tasks were performed at STABLE, made by Motekforce Link, present at the Motor Behavior Laboratory, at the School of Physical Education and Sport, of the University of São Paulo.
This equipment is composed by: three projectors, one audio system that provide lateral and frontal coverage, allowing a semi-immersive experience; one force platform of 1m²; a motion capture system and database of participants; a set of evaluation applications and stability and balance training tasks.
For the characterization of the EG were used MMSE (Bertolucci et al., 1994), Fugl-Meyer Scale (Fügl-Meyer, Jaasko, Leyman, Olsson, & Steglind, 1975) and Orpington Prognostic Scale (Lai, Duncan, & Keighley, 1998), and the characterization of the CG for done with MMSE scale.
MMSE is a test of cognitive function, composed of questions typically grouped into seven specific categories: time orientation, location orientation, 3-word registration, attention and calculation, memory of the 3 words, language and visual constructive capability. The MMSE score may range from 0 to 30 points, with a value less than 23 indicative of dementia (Bertolucci et al., 1994).
Fugl-Meyer scale is divided into 5 domains: Motor function, sensitivity, balance, range of motion and pain. The items are scored on an ordinal scale of 0 to 2 (0 = no performance, 1 = partially performed, 2 = complete performance), totaling 226 points (Fügl-Meyer et al., 1975).
The Orpington Prognostic Scale evaluates the severity of the stroke, it considers the evaluation of motor deficits in the upper limb, proprioception, balance and cognition, and through it, the cerebrovascular event can be categorized into mild (1.6 to 3.1 ), moderate (3.2 to 5.2) and severe (score greater than or equal to 5.3) (Lai et al., 1998).
Procedures
Initially, all of the subjects were evaluated by MMSE (Bertolucci et al., 1994), and the EG were evaluated by the Fugl-Meyer (Fügl-Meyer et al., 1975) and Orpington Prognostic (Lai et al., 1998) scales too.
After the characterization with these scales, both EG and CG were submitted to eight sessions of task’s practice in VR environment.
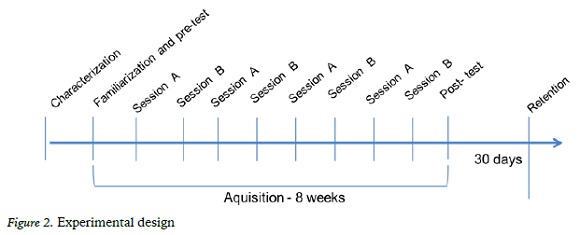
On the first day of practice, each task was demonstrated to the study participants by an experienced examiner. Subsequently, for each task, the individuals practiced two trials to familiarize themselves with the game, with movement and posture corrections through manual guidance and verbal commands. On the same day, the participants performed a block of three attempts from each of the eight games, which were considered as a pre-test and were performed without the examiner intervention.
Each session of the acquisition phase was one hour long, once a week.
Eight tasks were performed in a varied randomized way, four tasks at each week, and three attempts per session. The session A was composed of the tasks 2 D Maze 1, Balloon Pop, City Ride and Hit the Knees, and the session B was composed of the tasks Hit the Mole, Road Stepping, Road Encounters and Paper Flight.
At the end of the acquisition phase, participants performed a block of three trials from each of the eight games, which were considered post-test and were performed without examiner intervention to record the score and future analysis of participants’ performance. The retention test was performed in the same way one month after the end of the practice. The design is shown in Figure 2.
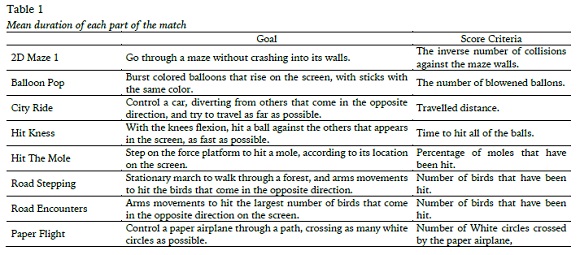
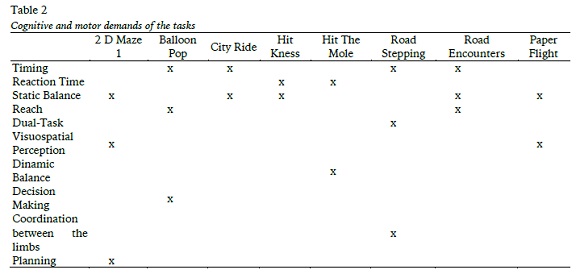
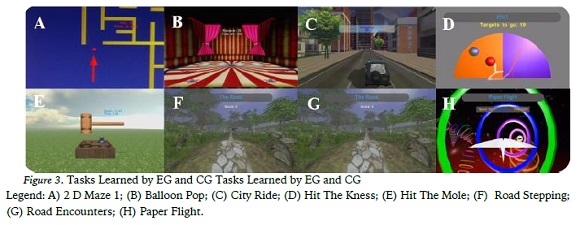
The description of each of tasks, according to its goals and score criteria are in the table below (Table 1). The cognitive and motor demands of each task were classified according to Cairolli et al. (2017), and they are described at the Table 2.
Each one of the eight tasks are represented at the Figure 3.
Statistical analysis
The dependent variable used to evaluate the performance in the pre-test, post-test and retention after thirty (30) days was the score achieved in each of the eight tasks practiced.
Demographic data and clinical characteristics of the participants of both groups were compared using the t-test for independent samples.
Tests of normality and homogeneity of variance were performed, using the Kolmogorov- Smirnov and Levene test, respectively. Moreover, as normality assumptions were reached, inferential analysis of the pre-test, post-test, and retention was performed using the Multiple Comparison Analysis of Variance (3x2), with Tukey post hoc.
The alpha considered was 0.05, and it was verified each power analysis (P).
RESULTS
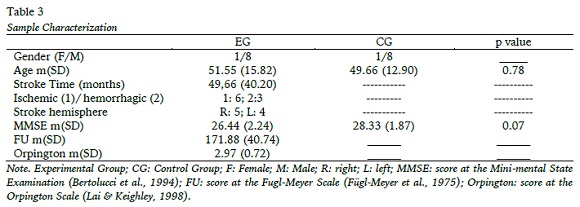
The sample characterization is represented in the Table 3. Both groups were similar for age, gender and cognitive functions. The EG does not present motor impairments and the stroke can be considered mild.
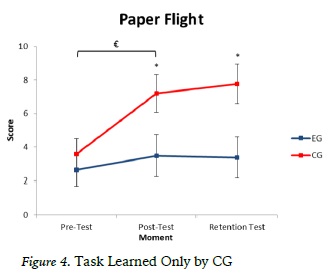
There was significant difference between the pre-test and post-test, and between the pre-test and the retention after 30 days, for both groups, in the City Ride (F= 18,96 p= 0.00; ES= 1.000), Hit Knees (F= 312,63; p= 0.53; ES= 0.148) and Balloon Pop (F= 8,31; p= 0.000; ES= 0.998). In the Figure 3 are represented the performances of both EG and CG, in each moment, for each of the three tasks learned by both groups. The task learned only by CG was Paper Flight.
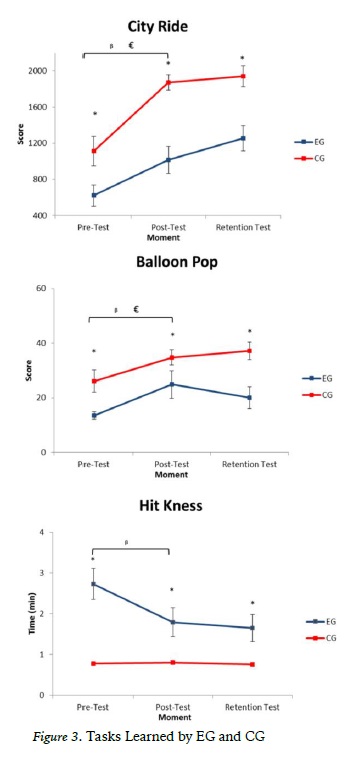
Through the Figure 3 it is possible to identify that both groups were different (p= 0.03; ES= 0.566), and there were interaction effects between moment and group factors (p=0.05; ES= 0.569). The post hoc found differences between the groups in the post-test (p= 0.04) and retention (p= 0.02) moments. Related to the intragroup analysis, it was found a significant difference (p=0.003; ES=0.905) between pre- test and post-test only for CG (F= 2,31; p= 0.018; ES= 0.700). These results are represented in the figure below (figure 4).
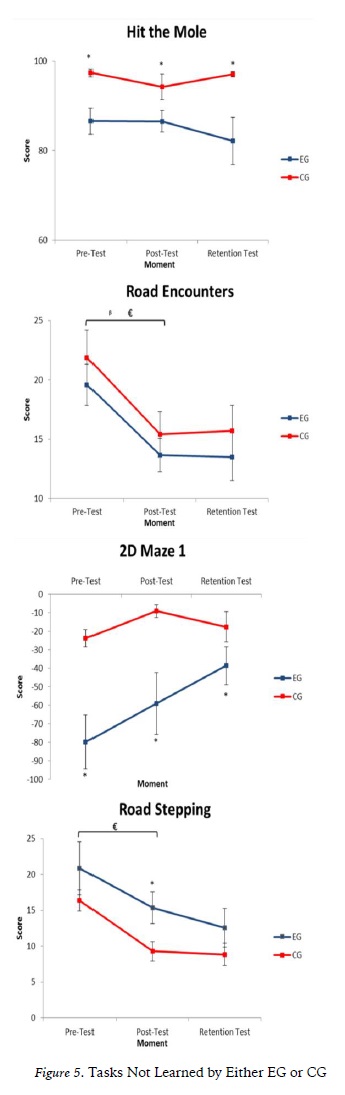
The tasks which neither EG or CG learned were: Hit The Mole (F= 200,74; p= 0.30; ES= 0.251), Road Stepping (F= 5,79; p=0.00; ES=1.000), 2D Maze 1 (F= 2,42; p= 0.009; ES=0.791), e Road Encounters (F= 14,75; p= 0.001; ES= 0.959). There was no significant difference for both groups between the pre-test and post- test performance in those tasks, or even if there was, the same was not sustained in the retention test, after thirty days (figure 5).
DISCUSSION
The aim of the present study was to investigate the motor learning process of a sample of VR tasks, with different demands, in post stroke individuals, and compare it with healthy subjects.
Both groups were able to learn three of the eight practiced tasks: Balloon Pop, City Ride and Hit Knees. Only one task was learned exclusively by CG: Paper Flight. While four of them were not learned by neither group: Hit The Mole, 2 D Maze 1, Road Stepping e Road Encounters.
It is known that the brain stimulation process of post stroke individuals can be affected, leading to changes in its functions, such as the ability to understand task goals, and process important information for planning and implementation ( Torriani-Pasin, 2010).
Despite that, studies have shown that post- stroke individuals are capable to learn tasks (Boyd et al., 2007; Winstein, Merians, & Sullivan, 1999), even those practiced in VR’s environment (Bonuzzi et al., 2016). In addiction it is known that, for individuals affected by a mild stroke (Hanlon, 1996) such as the subjects of the present study, it is suggested a varied practice, whether randomized or in block, because it allows a greater retention and generalization of the learned content, when compared to the constant practice (Winstein et al., 1999).
However, not only the practice characteristics are capable to affect the motor learning process, but also the characteristics of the stroke and of the task practiced (Boyd et al., 2009; Torriani- Pasin, 2010). In the present study, the specific element that was different in each of the eight tasks, and maybe affected the motor learning process was the task’s level of complexity. The complexity of a task is determined by its quantity and types of motor and cognitive demands, the processing demand of information (Naylor & Briggs, 1963) and the quantity of attention needed (Magill, 2011). Billing (1980) classified the task’s complexity with four different aspects: perception, decision-making, motor act and feedback.
Perceptual complexity is related to the perception and interaction of different stimulus, and can be defined by the quantity of stimulus needed to perform a task, its duration, and a possible interaction of the task over them, as the intensity of this interaction. Decision-making corresponds to the action of choosing the most appropriate response, its velocity, and the number of decisions that must be done. Motor act it is associated to the number of movement’s degrees of freedom, speed and precision. While the feedback aspect is defined by the quantity, quality and accuracy of the information which the individuals have the access to.
Pohl and Winstein (1999) showed that, when it comes to a fine motor task that involves upper limbs reach, with different levels of complexity, post stroke individuals are able to reduce their time of performance in both low and high levels of complexity. However, they presented a worse performance when compared to healthy subjects. With a postural control task, in VR environment, Bonuzzi et al (2016) found that task’s complexity affects, in a higher intensity, individuals with right hemisphere lesions. Palma (2016) investigated the motor learning process of a task involving the displacement of the center of pressure, with different levels of complexity, number of elements and processing load. Post stroke individuals presented similar performances as healthy subjects in a low complexity task (no inter-group difference), being able to learn it in a similar way as CG. However, their task performance times were higher in all of the assessed moments. In addition, for the higher complexity tasks, post stroke individuals were not able to learn it, presenting both score and performance time worse than the healthy subjects.
In the present study, the tasks demands were dual-task, precision, stability (static or dynamic), planning, visuospatial perception, timing, reaction time, decision-making, coordination between the limbs and reach.
For the motor act aspect, the results of the present study resemble to Billing (1980) determinations. The more complex tasks were those involving higher levels of precision and movement speed such as 2D Maze 1 (required high levels of precision to displace the center of pressure), Road Stepping and Hit the Mole, (involves faster body’s movements and precision), Road Encounters (with a high demand of accuracy of upper limb movements). Those tasks were not learned by any of both groups.
Finally, to the decision-making aspect, in the tasks without a great demand for decision- making velocity and that involved timing or planning, such as Balloon Pop and City Ride, the complexity levels were lower, and both groups were able to learn. When a dual-task was required, such as in Road Stepping, the attention’s division between the stationary gait and upper limb’s reach affected the motor learning process of both groups that were not able to learn this task with only four sessions of practice. This results can be justified according to Fitts and Posner (1967), as it is only possible to introduce a second task without affecting the performance of the first one if the third phase of the motor learning process (Autonomous phase) was achieved in the first ability.
The task learned only by CG involved displacement of the center of pressure (CP) and visuospatial perception. However, unlike 2D Maze 1, the demand for movement accuracy was moderate, such as its task complexity level, and errors related to the displacement of the CP did not necessarily cause score reductions.
These results supports Boyd et al. (2007), as chronic post stroke individuals are able to improve their performances in different tasks, through the practice, being only affected to the improvement magnitude by the complexity of the task. These individuals did not learn tasks with a moderate or a high level of complexity. Further studies are necessary to investigate if with a longer acquisition phase, post stroke individuals are able to learn moderate and high complex tasks in similar ways as healthy subjects and monitor the quality of movement and the non- realization of compensation.
CONCLUSION
Post stroke individuals are able to learn VR’s tasks with low complexity levels (involving decision-making velocity, timing and planning) such as healthy subjects. However, this does not occur when it comes to tasks with moderate or higher levels of complexity (demanding dual-task, higher levels of precision and movement speed).
REFERENCES
Adkins, D. L., Boychuk, J., Remple, M. S., & Kleim, J. a. (2006). Motor training induces experience- specific patterns of plasticity across motor cortex and spinal cord. Journal of Applied Physiology, 101(6), 1776-1782. http://doi.org/10.1152/japplphysiol.00515.2006 [ Links ]
Aminov, A., Rogers, J. M., Middleton, S.,Caeyenberghs, K., & Wilson, P. H. (2018). What do randomized controlled trials say about virtual rehabilitation in stroke? A systematic literature review and meta-analysis of upper-limb and cognitive outcomes. Journal of Neuroengineering and Rehabilitation, 15(1), 1-29. [ Links ]
Bertolucci, P. H., Brucki, S. M., Campacci, S. R., & Juliano, Y. (1994). O Mini-Exame do Estado Mental em uma população geral. Impacto da escolaridade. Arquivos de Neuro-Psiquiatria, 52(1), 1-7. http://doi.org/10.1590/S0004-282X1994000100001 [ Links ]
Billing, J. (1980). An Overview of Task Complexity. Motor Skills: Theory into Practice, 4(1), 18-23. [ Links ]
Bonuzzi, G. M. G., Freitas, T. B., Corrêa, U. C., Freudenheim, A. M., Pompeu, J. E., & Torriani- Pasin, C. (2016). Learning of a postural control task by elderly post-stroke patients. Motricidade, 12(1). http://doi.org/10.6063/motricidade.7004 [ Links ]
Boyd, L. A., Edwards, J. D., Siengsukon, C. S., Vidoni,E. D., Wessel, B. D., & Linsdell, M. A. (2009). Motor sequence chunking is impaired by basal ganglia stroke. Neurobiology of Learning and Memory, 92(1), 35-44. http://doi.org/10.1016/j.nlm.2009.02.009 [ Links ]
Boyd, L. A., & Winstein, C. J. (2001). Implicit motor- sequence learning in humans following unilateral stroke: The impact of practice and explicit knowledge. Neuroscience Letters, 298(1), 65-69. http://doi.org/10.1016/S0304-3940(00)01734-1 [ Links ]
Boyd, L. A., & Winstein, C. J. (2004). Cerebellar stroke impairs temporal but not spatial accuracy during implicit motor learning. Neurorehabilitation and Neural Repair, 18(3), 134-43.http://doi.org/10.1177/0888439004269072 [ Links ]
Boyd, L. a, Quaney, B. M., Pohl, P. S., & Winstein, C.J. (2007). Learning implicitly: effects of task and severity after stroke. Neurorehabilitation and Neural Repair, 21(5), 444-454. http://doi.org/10.1177/1545968307300438
Cho, K. H., Lee, K. J., & Song, C. H. (2012). Virtual-Reality Balance Training with a Video-Game System Improves Dynamic Balance in Chronic Stroke Patients. The Tohoku Journal of Experimental Medicine, 228(1), 69-74. [ Links ]
Cirstea, C. M., Ptito, A., & Levin, M. F. (2006). Feedback and cognition in arm motor skill reacquisition after stroke. Stroke; a Journal of Cerebral Circulation, 37(5), 1237-42. http://doi.org/10.1161/01.STR.0000217417.89347.63 [ Links ]
da Silva Cameirão, M., Badia, B. I., Duarte, E., & Verschure, P. (2011). Virtual reality based rehabilitation speeds up functional recovery of the upper extremities after stroke : A randomized controlled pilot study in the acute phase of stroke using the Rehabilitation Gaming System. Restorative Neurology and Neuroscience, 29, 287-298. http://doi.org/10.3233/RNN-2011-0599 [ Links ]
Eerdt, T. J. B., Dawes, H., Sackley, C., Izadi, H.,Bovend, A., Tj, E., … Izadi, H. (2010). An Integrated Motor Imagery Program to Improve Functional Task Performance in Neurorehabilitation : A Single-Blind. Archives of Physical Medicine and Rehabilitation, 91(6), 939-946. http://doi.org/10.1016/j.apmr.2010.03.008
Fitts, P. M., & Posner, M. I. (1967). Human performance. Oxford, England: Brooks/Cole. [ Links ]
Fügl-Meyer, A. R., Jaasko, L., Leyman, I., Olsson, S., & Steglind, S. (1975). The post-stroke hemiplegic patient. Scand J Rehabil Med, 7, 13-21. [ Links ]
Hanlon, R. E. (1996). Motor learning following unilateral stroke. Archives of Physical Medicine and Rehabilitation, 77(8), 811-5. [ Links ]
Holden, M. K. (2005). Virtual environments for motor rehabilitation: review. Cyberpsychology & Behavior, 8(3), 187-211. [ Links ]
Ioffe, M. E., Chernikova, L. a., Umarova, R. M., Katsuba, N. a., & Kulikov, M. a. (2010). Learning postural tasks in hemiparetic patients with lesions of left versus right hemisphere. Experimental Brain Research, 201(4), 753-761. http://doi.org/10.1007/s00221-009-2091-z [ Links ]
Kitago, T., & Krakauer, J. W. (2013). Motor learning principles for neurorehabilitation. Handbook of Clinical Neurology, 110, 93-103. doi: 10.1016/B978-0-444-52901-5.00008-3 [ Links ]
Lai, S. M., Duncan, P. W., & Keighley, J. (1998). Prediction of functional outcome after stroke: comparison of the Orpington Prognostic Scale and the NIH Stroke Scale. Stroke, 29(9), 1838- 1842. http://doi.org/10.1161/01.STR.29.9.1838 [ Links ]
Laver, K. E., George, S., Thomas, S., Deutsch, J. E., & Crotty, M. (2015). Virtual reality for stroke rehabilitation. Cochrane Database of Systematic Reviews, 9(2), 1-110. http://doi.org/10.1002/14651858.CD008349.pub2 [ Links ]
Laver, K. E., Lange, B., George, S., Deutsch, J. E., Saposnik, G., & Crotty, M. (2017). Virtual reality for stroke rehabilitation. Cochrane Database of Systematic Reviews, 96(10), 1508-1513. http://doi.org/10.1002/14651858.CD008349.pub4 [ Links ]
Magill, R. A. (2011). Aprendizagem e controle motor: conceitos e aplicações - (8th ed.). São Paulo: Phorte Editora. [ Links ]
Mendes, F. A. S., Pompeu, J. E., Lobo, A. M., da Silva,K. G., Oliveira, T. de P., Zomignani, A. P., & Piemonte, M. E. P. (2012). Motor learning, retention and transfer after virtual-reality-based training in Parkinson’s disease - effect of motor and cognitive demands of games: a longitudinal, controlled clinical study. Physiotherapy, 98(3), 217-223. http://doi.org/10.1016/j.physio.2012.06.001
Naylor, J. C., & Briggs, G. E. (1963). Effects of task complexity and task organization on the relative efficiency of part and whole training methods. Journal of Experimental Psychology, 65(3), 217-224. http://doi.org/10.1037/h0041060 [ Links ]
Palma, G. C. dos S. (2016). Aprendizagem de uma habilidade motora com diferentes níveis de complexidade em sujeitos pós acidente vascular cerebral (Dissertação de Mestrado, Escola de Educação Física e Esporte). http://doi.org/10.11606/D.39.2017.tde-13022017-114907 [ Links ]
Platz, T., Denzler, P., Kaden, B., & Mauritz, K.-H. (1994). Motor learning after recovery from hemiparesis. Neuropsychologia, 32(10), 1209-1223. http://doi.org/10.1016/0028-3932(94)90103-1 [ Links ]
Pohl, P. S., & Winstein, C. J. (1999). Practice effects on the less-affected upper extremity after stroke. Archives of Physical Medicine and Rehabilitation, 80(6), 668-675. [ Links ]
Pompeu, J. E., Alonso, T. H., Masson, I. B., Maria, S., Pompeu, A. A., & Torriani-pasin, C. (2014). The effects of virtual reality on stroke rehabilitation: A systematic review. Motricidade, 10(4), 111-122. [ Links ]
Torriani-Pasin, C. (2010). Aprendizagem de uma habilidade motora com demanda de planejamento em sujeitos pós Acidente Vascular Encefálico em função do lado da lesão., 172. Retrieved from http://www.teses.usp.br/teses/disponiveis/39/39132/tde-16082010-153057/pt-br.php [ Links ]
Torriani-Pasin, C., Bonuzzi, G., Palma, G., Freudenheim, A., & Corrêa, U. (2018). Motor learning in post stroke subjects: the effects of practice conditions on the temporal synchronization. Motriz. Revista de Educacao Fisica, 24(2), 1-9. [ Links ]
Torriani-Pasin, C., Palma, G. C. dos S., & Freitas, T. B. de. (2016). Aprendizagem Motora após lesão encefálica no paciente adulto: aplicabilidade na reabilitação. In C. Garcia & L. Facchinetti (Eds.), Associação Brasileira de Fisioterapia Neurofuncional (Ciclo 3, pp. 131-184). Porto Alegre: Artmed Panamericana.
Winstein, C. J., Merians, A. S., & Sullivan, K. J. (1999). Motor learning after unilateral brain damage. Neuropsychologia. [ Links ]
Acknowledgments: Nothing to declare.
Conflict of interests: Nothing to declare.
Funding: Nothing to declare.
Manuscript received at August 22nd 2018; Accepted at February 10th 2019
[*]Corresponding author: School of Physical Education and Sport, of the University of São Paulo - Professor Mello Moraes Avenue, 65 - Email: tatibeline@gmail.com

