











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkEctopic interstitial pregnancy is a rare entity with an estimated incidence of 2-6% of all ectopic pregnancies and occurs in the proximal intramural section of the fallopian tube1. The known predisposing factors include salpingectomy, pelvic inflammatory disease, pelvic surgery, previous ectopic pregnancy, uterine anomalies or tumors and in vitro fertilization. Due to myometrial distensibility they tend to appear considerably late and a cornual rupture can lead to a catastrophic hemorrhage1,2. The mortality rate is 2-2.5% and is seven times higher than all other ectopic pregnancies1,2.
The high sensitivity of ultrasound makes it the preferred initial method of diagnosis1. The ultrasound findings include an empty uterine cavity and the presence of eccentrically located gestational sac (GS) at the uterine fundus at least 10mm from the lateral edge of the uterine cavity and surrounded by myometrial tissue3.
We present a case of a spontaneous interstitial ectopic pregnancy ipsilateral to a prior adnexectomy.
A 25-year-old woman with history of two previous abortions and a prior left laparoscopic adnexectomy for ovary torsion presented to the emergency room with abdominal pain and 8 weeks of amenorrhea. The patient was haemodynamically stable and had left lower quadrant pain. On transvaginal ultrasound, a thick and hyperechogenic endometrial lining was seen and no intrauterine GS could be found. A GS with an embryo with a crown-rump length of 10.3mm and cardiac activity was identified in the left cornual area (Figure 1), corresponding to a 7 week pregnancy. In a transverse plane at the uterine fundus it became clear that the GS was located 11mm from the uterine cavity, in the intramural portion of the tube (Figure 2). As expected from the patient’s history we could not identify the left ovary. A corpus luteum image was seen in the right ovary.

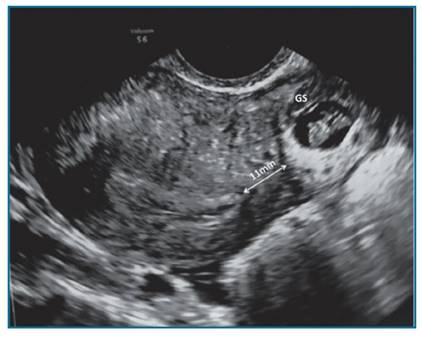
FIGURE 2 Ultrasound transverse plane at the uterine fundus. Gestational sac (GS) located in the interstitial portion of the fallopian tube, 11mm from the uterine cavity, surrounded by myometrium.
A laparoscopic surgery was performed and no remanescent left fallopian tube was seen. A left cornual resection was successfully performed without complications.
About one-third of spontaneous pregnancies in women with previous salpingectomy can result from oocyte transperitoneal migration to the contralateral fallopian tube4. The present case enhances the possibility of intrauterine transmigration of a fertilized egg as an etiology of spontaneous ectopic pregnancy. Therefore, the occurrence of ectopic pregnancy even after a complete resection of ipsilateral fallopian tube is still a possible event.
Patient inform consent was obtained.

