










Serviços Personalizados
Journal

Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
 Citado por SciELO
Citado por SciELO Links relacionados
 Similares em
SciELO
Similares em
SciELO Compartilhar

 Permalink
PermalinkRevista Portuguesa de Enfermagem de Saúde Mental
versão impressa ISSN 1647-2160
Revista Portuguesa de Enfermagem de Saúde Mental no.14 Porto dez. 2015
https://doi.org/10.19131/rpesm.0100
ARTIGO DE INVESTIGAÇÃO
Quality of life and care burden among informal caregivers of elderly dependents in Catalonia
Qualidade de vida e carga sobre cuidadores informais de idosos dependentes na Catalunha
Calidad de vida y carga en los cuidadores informales de personas mayores dependientes en Cataluña
Montserrat Puig*, Núria Rodriguez**, Maria Teresa Lluch-Canut***, Carmen Moreno****, Juan Roldán*****, Pilar Montesó******
*PhD; Nurse; Professor at the University of Barcelona, School of Nursing, Mental Health Sciences Department, Feixa Llarga, s/n, 08907 Hospitalet de Llobregat, Barcelona, Spain. E-mail: monpuigllob@ub.edu
**PhD; Professor of Sociology of Organizations at the University of Barcelona, Faculty of Economics, 08034 Barcelona, Spain. E-mail: nrodriguez@ub.edu
***Nurse; Professor at the University of Barcelona, School of Nursing, Mental Health Sciences Department, 08907 Hospitalet de Llobregat, Barcelona, Spain. E-mail: tlluch@ub.edu
****Nurse; Professor at the University of Barcelona, School of Nursing, Department of Fundamental Care and Medical-Surgical Nursing, 08907 Hospitalet de Llobregat, Barcelona, Spain. E-mail: carmenmoreno@ub.edu
*****PhD; Nurse; Professor at University of Barcelona, School of Nursing, Campus Docent Sant Joan de Déu-Fundació Privada, 08950 Esplugues de Llobregat, Barcelona, Spain. E-mail: JRoldan@santjoandedeu.edu.es
******PhD; Nurse; Professor at Rovira i Virgili University of Tarragona, Faculty of Nursing, 43003 Tarragona, Spain. E-mail: mariapilar.monteso@urv.cat
ABSTRACT
INTRODUCTION: The Quality of Life (QOL) of primary caregivers may have decreased. The aim of this study was to assess the objective and subjective elements related to QOL of the primary caregivers of the dependent elderly. The theoretical framework used was the role theory and socialization process of care and the theory of social disengagement.
METHODOLOGY: Qualitative study. The sample consisted of n=22 informal caregivers of people over 75 years old treated by the Primary Home Care Service Center of Vilafranca del Penedes (Barcelona, Spain). Dimensions used were: socio-demographic data, quality of life and happiness, care burden, social and family relationships, motivation and feelings when caring and the health status of the caregiver. The technique chosen was a semi-structured interview.
RESULTS: In our study, half of the caregivers had a regular perception of health and QOL, care burden, a self-care deficit and contradictory feelings towards caring.
CONCLUSIONS: The Informal caregivers of dependent elderly of the home care program are mainly older women and with one or more chronic condition. They have a self-care deficit. They say they have little social and personal life.
Keywords: Burden; Informal caregivers; Elderly; Quality of life
RESUMO
INTRODUÇÃO: A qualidade de vida (QV) dos cuidadores primários pode ter diminuído. O objetivo deste estudo foi avaliar os elementos objetivos e subjetivos relacionados com a qualidade de vida dos cuidadores primários de idosos dependentes. O referencial teórico utilizado foi a teoria do papel e o processo de socialização dos cuidados e da teoria do desengajamento social.
METODOLOGIA: Estudo qualitativo. A amostra é composta de n=22 cuidadores informais de pessoas com mais de 75 anos atendidos pelo Centro de Vilafranca del Penedès (Barcelona, Espanha) Atenção Básica. As dimensões utilizadas foram: demográfico, a qualidade de vida e felicidade, sobrecarga, relações sociais e familiares, a motivação e os sentimentos de cuidado e a saúde do cuidador. A técnica escolhida foi a entrevista semi-estruturada.
RESULTADOS: Em nosso estudo, metade dos cuidadores tinha uma percepção regular de saúde e qualidade de vida, a carga de cuidados, déficit de autocuidado e sentimentos contraditórios para o cuidado.
CONCLUSÕES: Os cuidadores informais de programa de atenção domiciliar de idosos dependentes são mulheres, principalmente idosos com uma ou mais condições crônicas. Têm um déficit de autocuidado. Expressaram pouca vida social e pessoal.
Palavras-Chave: Carga; Cuidadores informais; Idosos; Qualidade de vida
RESUMEN
INTRODUCCIÓN: La calidad de vida (CV) de los cuidadores principales puede estar disminuida. El objetivo de este estudio fue evaluar los elementos objetivos y subjetivos relacionados con la calidad de vida de los cuidadores principales de las personas mayores dependientes. El marco teórico utilizado fue la teoría del rol y el proceso de socialización de los cuidados y la teoría de la desvinculación social.
METODOLOGÍA: Estudio cualitativo. La muestra está formada por n=22 cuidadores informales de personas mayores de 75 años atendidos por el Centro de Atención Primaria de Vilafranca del Penedès (Barcelona, España). Las dimensiones utilizados fueron: datos sociodemográficos, calidad de vida y la felicidad, la sobrecarga, las relaciones sociales y familiares, la motivación y los sentimientos en el cuidado y el estado de salud del cuidador. La técnica elegida fue una entrevista semi-estructurada.
RESULTADOS: En nuestro estudio, la mitad de los cuidadores tenían una percepción de salud y calidad de vida regular, carga asistencial, déficit de autocuidado y sentimientos contradictorios hacia el cuidado.
CONCLUSIONES: Los cuidadores informales de personas mayores dependientes del programa de atención domiciliaria son principalmente mujeres de edad avanzada y con una o más condiciones crónicas. Tienen un déficit de autocuidado. Expresan tener poca vida social y personal.
Palabras Clave: Carga; Cuidadores informales; Personas mayores; Calidad de vida
Background
The role of women as caregivers is related to tradition, socialization and economic relations that place women as caretaker of the family institution. So that care is part of their life (Campo, 2000). In the caregiving process to a sick person or with high dependency, the primary caregiver has some conflicting feelings of positive and negative characteristics (Campo, 2000). The positive feelings are the identification of emotional well-being, self-acceptance, autonomy, control of the environment, the cultural significance of care and reciprocity. Moreover, according to some studies, the desire to care for and help the dependent person can reduce stress in the caregiver (Farran, 1997). This lets you see the care from a constructivist and artisan's perspective, made with with and love (De la Cuesta, 2004). When caring is done from this perspective the caregivers perceive a better quality of life (QOL) than people who see care as a burden or obligation. As negative feelings, the primary caregiver can have different types of emotional reactions: guilt, anger, helplessness, shame, sadness, depression, loneliness and stress. Some caregivers experience changes in health status: fatigue, headaches, back pmain, insomnia, stress, depression, anxiety and impaired self-perceived health; this can also cause care to be an burden, which is expressed as physical and emotional exhaustion (Cox, Walker, Mildred & Hognstel, 2006; Marquez, Bustamante, Kozey-Keadles, Kraemer & Carrion, 2012), in other words, this is known as the burden or caregiver's syndrome.The QOL of the primary caregiver of a dependent elderly person can be altered for different reasons and costs. The informal care costs are related to employment, social, family, economic, legal, leisure and health issues (Campo, 2000). Furthermore, most caregivers are women who should consider the dilemma of work or care (Campo, 2000). The theoretical framework used were the role theory and socialization of care and the theory of social disengagement. Parsons attributed to the functioning of a person in society according to the different social roles that should perfom in this case the sick role and the role of elder by the role theory (Parsons, 1999). Theory of social disengagement explains that elderly moves away from the social life and society offers less chance, so older people adapt to their social position (Cummings & Henry, 1961).
For this reason, the stated objective of this study was to evaluate the elements involved in the quality of life in primary caregivers of the dependent elderly, identifying if care is a burden.
Method
Participants
The area of study was the Primary Care Center of Basic Health Area in Vilafranca (Barcelona, Spain). The methodology used was a case study (Bonache, 1999). The study populations were primary caregivers of persons over 75 years old treated by the Home Care Service area of the center, as this was the group that had more dependency and care needs. The patients we studied had cognitive impairment, had a moderate level of dependence according to the Barthel Index. Most patients need help to take a bath or shower, walk or move as the Katz index and some difficulty as the Lawton index for dining and shopping activities. The main pathologies were suffering from skeletal muscle, cardiovascular, endocrine, pulmonary and digestive, and 89% (n=19) of the elderly had multiple disorders and taking more than one medication. Daily care is provided about 7 hours a day, although most needed help during the night.
Material and Procedure
The population study was elderly over 75 years old treated by the Home Care Service at the Primary Care Center in Vilafranca (Barcelona, Spain); we established the study sample choosing convenience sampling criteria. A sample of n=22 informal caregivers. The criteria for inclusion in the sample were: to have been the primary caregiver, for at least two years, of a person aged 75 and over treated by the home care program of the Primary Care Center in Vilafranca and agreeing to participate in the study. The exclusion criteria were not having behavioural and cognitive symptoms. To access the sample, permission was obtained from the maximum health agency that exists in the autonomous community of Catalonia, the Catalan Institute of Health (ICS).
Measurement
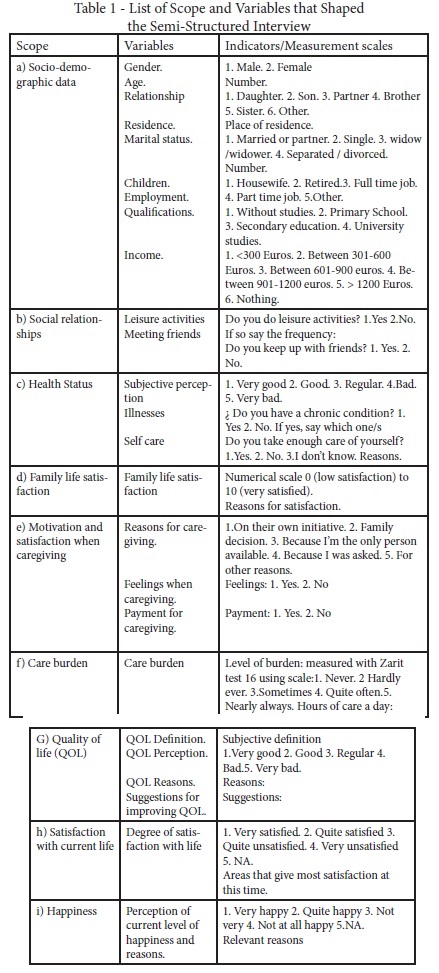
The scope analyzed was: a) socio-demographic data, b) social relations, c) health status of the caregiver, d) satisfaction with regard to family life, e) motivation and feelings about caring, f) care as a burden, g) QOL, h) life satisfaction and i) perception of happiness. The technique chosen was a semi-structured interview conducted by the researcher in the caregiver's home, and recorded with the permission of the interviewee, following a telephone appointment from data provided by the nurses in the home care service. The tool used to conduct the semi-structured interview is shown in Table 1. To elaborate, questions which had been validated by the Sociology Research Center5 and the World Organization Health (OMS, 2000), were taken into account as well as the Zarit test to determine the level of burden in care (Martín et al., 1996). This test has 22 items. The cutoff points are: <46 No burden; 46-47 to 55-56 Slight burden; > 55-56 Extreme burden. This test is used a generic in Primary Care in Catalonia for all caregivers. Burden was assessed with other variables from the interview. A trial run was carried out before interviewing the caregivers of the study.
Data Analysis
For quantitative variables descriptive analyses (frequencies and percentages) and measures (mean and range) were carried out. Qualitative variables were analyzed from basic descriptive measures (frequencies and percentages). For qualitative analysis interviews were transcribed and the dimensions are grouped by categories, encoding them and relating them by topic.
Sampling Characteristics
The mean age of the caregivers was X = 64 years (range 54-79 years). Women accounted for 72.7% (n=16) of all caregivers. In first place, daughters were the primary caregivers. Spouses were second, in third place sons and other relatives were last. 95% (n=21) of caregivers lived in the same city as the elderly person they were caring for and also many lived in the same district. 77.3% were married and 81.8% had children. The perceived health status was 50% in normal cases (Table 2). On the other hand, 90.9% of the individuals studied had at least one chronic condition.
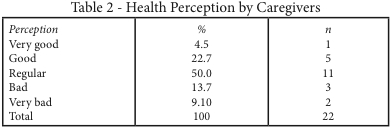
In the table 2, 67.3% (n=14) of the individuals studied were not working due to the advanced age of the caregiver, his/her choice to care or the impossibility of combining work and care of the dependent elderly. Regarding the level of education 68.2% had a low level of education. The total income was low to moderate, only one caregiver had an income of more than 1200 Euros per month and three did not receive any pension.
Results
Social and Family Relationships
Social relations were scarce, given that 95% never took part in leisure outings. The little free time was used primarily to be at home, watching TV and/or reading. All caregivers expressed the need for more time for leisure activities. In assessing satisfaction with family life, on a scale of 0-10, 67.3% were satisfied with a score of 8 points or more. 86.4% (n=19) felt valued by the people they cared for: they felt this because the person cared for verbally expressed their gratitude and had no complaints about care. Caregivers, who do not feel valued, expressed that this was due to the demands and dissatisfaction of the elderly person regarding the care provided.
Motivation and Burden in Care
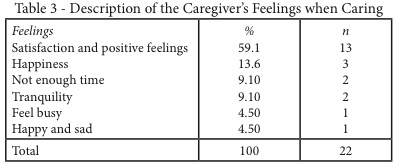
Among the reasons caregivers gave for looking after their elderly, it stands out that the majority care on their own initiative, feel satisfied doing the caring and would feel bad if they didn't do it as for many of them their duty is to look after the people in their family. With regard to identifying whether they received any financial compensation for caring for a dependent elderly person, the results showed that 90.9% (n=20) were not paid for caring. As for the perceived feelings about caring, 81.8% (n=18) had positive feelings when doing care work (Table 3). With regard to determining if care was a burden according to the Zarit test, the maximum score was 37 points, which means that they did not show care to be a burden, as the results were not higher than 46 points (the score at which it is considered a burden). However, they reported having little free time and spending X = 6.9 hours a day looking after the elderly person, means little sleep, little rest and do not make a balanced diet. They also expressed that they didn't look after themselves enough due to a lack of time for their personal lives.
Quality of Life, Satisfaction and Happiness
It was difficult to establish a subjective definition of quality of life. 77.2% (n=17) emphasized health as an important matter. In some definitions, this was expressed exclusively and in others it was joined with other concepts, such as: having money and resources, having good relationships, having love, having autonomy, having a job and having time for you, such as these phrases:
"Having good health and family relations" (E.20)
"Do what you want, have health and resources" (E.19)
"Take time to enjoy and be good about oneself" (E.04)
When analyzing the perception of quality of life, the most frequent response was that of a good quality of life (see Table 4).
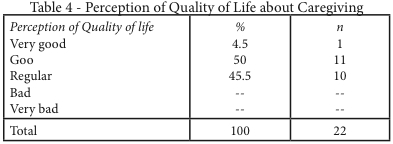
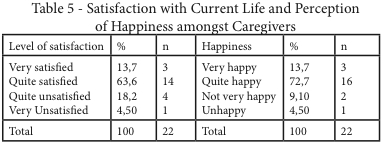
The perception of the quality of life as good or very good was related to being healthy, satisfied and happy about being a caregiver, having good family relationships and geriatric resources. The perception of a fair or poor quality of life was related to poor health, and not having much social relationship. Psychological problems that were expressed and related to a poor or non-existent QOL were anxiety, depression and stress. With regard to determining the degree of life satisfaction, 77.2% (n=17) were satisfied (see Table 5). Regarding the aspects that gave them most satisfaction at present, aspects relating to the family (having good family relationships and family health) stood out most; other aspects were being the caregiver, having free time, being able to read and study and maintain relationships with friends. Regarding the perception of happiness, 72.7% (n=16) reported feeling quite happy (see Table 5).
The proposals to improve their quality of life included having more freedom and more free time for their personal things. No relationship was found between the socio-demographic variables and a better perception of quality of life, nor with the life satisfaction and happiness variables. There was relationship found between the caregiver's perceived health and their perception of quality of life: the poor the health perception, the worse the perception of quality of life.
Discussion
Women are the primary caregivers. This data is still a fact that we have observed in other studies of caregivers, both in Spain and in other European countries (Crespo & López, 2007; Gallart, 2007). The place of residence of the elderly is near the primary caregiver, and thus, in dependency cases, the elderly is cared for by their immediate family. When the caregiver does not live near, the caregivers or the elderly move to nearby homes, to facilitate better contact and ultimately, a more personalized care. Having little time for leisure activities and being with friends is also shown in other national and international studies which stresses that the caregiver does not have time to enjoy themselves (Gallart, 2007; Pérez, 2006; Sequeira 2010; Sequeira, 2013). As in the Pinquart, Sorensen & Correlates (2007) and Tanner & Townsend-Rocchiccioli (Tanner, 2004) studies, caregivers in our study had a regular perception of their health status. A worse health status perception was related to a worse perception of QOL (Salin, Kaunonen & Astedt-Kurki, 2009). Also, the self-care deficit observed in our study sample is consistent with other studies (Bonache, 1999; Marquez et al., 2012; Pinquart et al., 2007;).On the other hand, women care on their own initiative and take on the role of primary caregivers mainly because they are women, as reflected in other studies (Pérez, 2006).The results are associated with the socialization of caregiving as the people who assume the role of carer feel identified as the caregiver and happier about doing the care work. However, this perception could change in the next generation of women, as they have fewer children and have them later, and the majorities do not want to give up work. Regarding care as a burden, the Zarit Test does not correctly reflect the reality of the caregivers in our study, since this test does not evaluate the actual level of burden in care. These caregivers have not directly expressed feeling burdened with care, however they do express having little time for leisure, social relationships, and a self-care deficit. This trend is also reflected in other studies (Sotto Mayor & Leite, 2011). In this sense, the results reinforce that informal caregivers of dependent persons may need assistance to have a break in their personal lives and take better care of their health. It will therefore be necessary to intervene to improve the QOL of primary caregivers (Pérez, 2006). The limitations of the study are on one hand the size of the sample is not representative as with qualitative studies and the study includes only dependents that they are served by the public health services of the city, leaving to study patients who are served by services private.
Conclusions
The Informal caregivers of dependent elderly of the home care program are mainly older women and with one or more chronic condition. They have a self-care deficit. They say they have little social and personal life. They do not perceive, nor express the real burden of care. They adapt to the current situation by having socialized the female caregiver's role. It is necessary to better inform caregivers about programs to aid dependency. It is advisable to develop self-management programs targeted at informal caregivers to reduce the burden of carrying out long-term care.
References
Bonache, J. (1999). El estudio de casos como estrategia de construcción teórica: Características, críticas y defensas. Cuadernos de Economía y Dirección de la Empresa, 3,123-140. [ Links ]
Campo, M. J. (2000). Apoyo informal a las personas mayores y el papel de la mujer cuidadora (ed. 31). Madrid: Opiniones y Actitudes, Centro de Investigaciones Sociológicas. [ Links ]
Cox, L., Walker, C., Mildred, C. H., & Hogstel, O. (2006). Educational needs of employed family caregivers of older adults: Evaluation of a workplace project. Geriatric Nursing, 27(3), 166-173. [ Links ]
Crespo, M., & López, J. (2007). El apoyo a los cuidadores de familiares mayores dependientes en el hogar: Desarrollo del programa. Madrid: Instituto de Mayores y Servicios Sociales. [ Links ]
De la Cuesta, C. (2004). Cuidado artesanal: La invención ante la adversidad. [ Links ] Colombia: Editorial Universidad de Antioquia.
Farran, C. J. (1997). Theoretical perspectives concerning positive aspects of caring for elderly persons with dementia: Stress/adaptation and existentialism. The Gerontologist, 37, 250-256. [ Links ]
Gallart, A. (2007). Sobrecarga del cuidador inmigrante no profesional formal en Barcelona (Tesis Doctoral). Universidad Internacional Cataluña, Barcelona, Spain. [ Links ]
Marquez, D., Bustamante, E., Kozey-Keadles, S., Kraemer, J., & Carrion, I, (2012). Physical activity and psychosocial and mental health of older caregivers and non-caregiver. Geriatric Nursing, 33(5), 358-364. [ Links ]
Martín, M., Salvadó, I., Nadal, S., Miji, L. C., Rico, J. M., Lanz, P., & Taussing, M. I. (1996). Adaptación para nuestro medio de la Escala de Sobrecarga del Cuidador (Caregiver Burden Interview) de Zarit. Revista de Gerontología, 6, 338-346. [ Links ]
Organización Mundial de la Salud (2000). Programa sobre envejecimiento y salud. Hacia un consenso internacional sobre los programas de cuidados de larga duración para las personas mayores. Ginebra: Organización Mundial de la Salud y Milbank Memorial Fund. [ Links ]
Pérez, A. (2006). El cuidador primario de familiares con dependencia: Calidad de vida, apoyo social y salud mental (Tesis Doctoral). Universidad de Salamanca, Salamanca, Spain. [ Links ]
Parsons, T. (1999). El sistema social. Madrid: Alianza. [ Links ]
Pinquart, M., & Sorensen, S. (2007). Correlates of physical health of informal caregivers: A meta-analysis. Journal of Gerontology: Psychological Sciences, 62, 126-137. [ Links ]
Salin, S., Kaunonen, M. & Astedt-Kurki, P. (2009). Informal carers of older family members: How they manage and what support they receive from respite care. Journal of Clinical Nursing, 18, 492-501. [ Links ]
Sequeira, C. (2010). Cuidar de idosos com dependência física e mental. Lisboa: Lidel. [ Links ]
Sequeira, C. (2013), Difficulties, coping strategies, satisfaction and burden in informal Portuguese caregivers. Journal of Clinical Nursing, 22: 491–500. doi: http://dx.doi.org/10.1111/jocn.12108
Sotto Mayor, M., & Leite, M. (2011). Implicações psicológicas da experiência informal de cuidar. Revista Portuguesa de Enfermagem de Saúde Mental (5), 37-44. [ Links ]
Tanner, J., & Townsend-Rocchiccioli, J. (2004). The perceived health of rural caregivers. Geriatric Nursing, 25(3), 145-214. [ Links ]
Recebido a 13 de março de 2015
Aceite para publicação a 20 de julho de 2015

