











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
A 53-year-old man presented to the otolaryngology clinic with a 2-month history of pharyngolaryngeal foreign body sensation, dysphagia and orthopnea. He had undergone cervical arthroplasty (levels C4-C5 and C5-C6) two years previously. Nasopharyngoscopy showed a round lesion on the right posterolateral hypopharygeal wall (Fig. 1), which decreased in size after swallowing and with modified Valsalva maneuver. Neck magnetic resonance imaging (MRI) revealed a T2-hyperintense cystic lesion (maximum diameter 29 mm), originated from the anterior longitudinal ligament of the cervical spine at C5-C6 level, bulging the retropharyngeal space (Fig. 2). The patient underwent excision of the cyst by right lateral cervicotomy, followed by implants removal and arthrodesis. Histologically, the cyst had a fibrotic wall, with no synovial cell lining and was filled with a gelatinous protein-rich fluid. Thus, confirming the diagnosis of a ganglion cyst. Symptoms were solved after the surgery and there was no recurrence after 1-year follow-up.
Ganglion cysts are benign lesions that originate from tendon sheaths and periarticular tissues, of degenerative, congenital or inflammatory etiology. They are typically found in peripheral joints. 1,2 Spinal ganglion cysts are rare, usually asymptomatic and mostly located in the dorsal portion of the spine. (3,4 Ventral location (in the anterior longitudinal ligament) associated with pharyngolaryngeal compression is an extremely rare finding. (5 MRI is the imaging method of choice, and histopathological assessment is required for establishing the definitive diagnosis of a ganglion cyst. 6 Treatment for symptomatic cases is surgical removal.
This case highlights that, despite being very rare, cervical ganglion cysts should be considered in the differential diagnosis of an anterior bulging of the posterior pharyngeal wall.
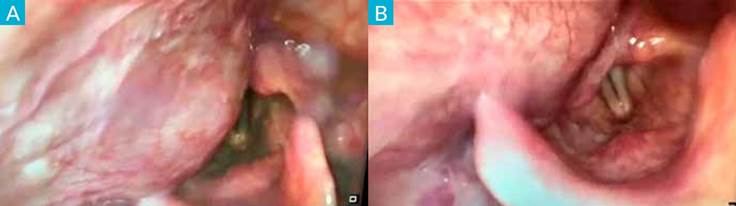
Figure 1 Nasopharyngoscopy demonstrating a round lesion on the right posterolateral hypopharygeal wall, with normal overlaying mucosa (A), which decreased in size after swallowing and with modified Valsalva maneuver (B).


