











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
Independence is understood as the person’s ability to carry out their activities of daily living, without the help of a third party. Therefore, it comprises the functional capacity for carrying out day-to-day tasks . Other authors also define it as self-care, pointing out that this self-care covers special care capacities, including bathing, eating, dressing, using the toilet, positioning, and transferring .
Analysis of the concept of independence and autonomy , concludes that the latter involves the concept of independence, since, as Beauchamp and Childress point out, independence allows the person to practice the right to freedom and authority arising from autonomy . It is essential to know their meanings, and as emphasized by Watson, the nurse, as the holder of knowledge and skills capable of responding to the needs of the person whom they care for, it is their concern to understand everything that involves and surrounds the concepts for its concretization, implementation, and monitoring. This knowledge assumes particular importance, when the goals of the professionals who care, focus especially on the rehabilitation of the person, whether at the physical, cognitive, psychological and/or social level.
Disease processes affect people's health and quality of life, who are their carriers. However, these repercussions may take on even more generous proportions if the person is hospitalized, since this, for several reasons, namely for bureaucratic and organizational aspects of care, promotes immobility processes, which contribute to dependency , especially in the elderly. The recovery of independence in these people, if there is no intervention, can be called into question , since immobility has consequences in all organic systems and in the elderly, due to their vulnerability, these assume greater severity .
People who experience independence, simultaneously refer to greater happiness and satisfaction with life, and consequently, greater quality of life .
In health-disease processes, the person loses and regains their independence, so it is necessary that health professionals, especially nurses, know the gains or losses in this area through its evaluation, being necessary to know the instruments available and their characteristics. To analyze and select the appropriate instrument, these professionals need to remember or know the limits of each concept they intend to develop, since this is the only way to direct their care and systematize it, aiming to realize their purposes.
Aware of this need and using a scoping review, it is intended to map the evidence to identify and analyze the instruments used to assess the person’s independence, which emerges from scientific production.
METHODOLOGY
The search for evidence using systematic review is at the heart of evidence-based practice in most scientific areas, especially in nursing. We opted for a scoping review. It is an investigation methodology that aims to map the existing scientific evidence implicit to an area of research and identify the inadequacies in the existing evidence .
The present study is a scoping review that sought to evaluate the existing evidence and to know the instruments used by health professionals to assess the person’s independence . Taking into consideration the knowledge that we wanted to synthesize, the review had as its starting point the following question: “What are the instruments used to assess the person’s independence?”.
Using the strategy: participants, concept and context (PCC), studies were included in the Scoping review that: a) address health professionals caring for the adult person; b) addressing the person’s independence; c) and using instruments to assess independence in all care settings; d) regarding the type of study, quantitative studies were examined. For this purpose, an electronic search was carried out in the Scopus, MEDLINE® (Medical Literature Analysis and Retrieval System Online) databases via PubMed, and CINAHL® (Cumulative Index to Nursing and Allied Health Literature) via EBSCO.
The research was developed in three stages. First, a limited search was conducted in the MEDLINE (via PubMed) and CINAHL (via EBSCO) databases to list the most commonly used words in the titles and abstracts of articles developed in the intended scientific area well as the indexing terms.
The second search was performed using the keywords and index terms identified, in the included databases, adapted according to the specificities of each database (Table 1). Finally, the list of references for each selected study was analyzed to include potential additional studies. Studies wrote in English, Spanish, and Portuguese, published between 2010 and 2020, were considered for inclusion in this review.
Table 1 Research strategy applied by database and the respective search results by database.
| Database: Scopus Filters: Excluding MEDLINE Results: 813 Search strategy (18 de abril de 2020) ( ( TITLE-ABS-KEY ( patient* ) ) AND ( TITLE-ABS-KEY ( independence ) OR TITLE-ABS-KEY ( autonomy ) ) AND ( ( TITLE-ABS-KEY ( theory ) OR TITLE-ABS-KEY ( concept ) ) ) ) AND NOT ( PMID ( 1* ) OR PMID ( 2* ) OR PMID ( 3* ) OR PMID ( 4* ) OR PMID ( 5* ) OR PMID ( 6* ) OR PMID ( 7* ) OR PMID ( 8* ) OR PMID ( 9* ) ) |
| Database: CINAHL complete (via EBSCO) Filters: Excluding MEDLINE Results: 313 Search strategy (18 de abril de 2020) S1 - MH Patients OR TI patient* OR AB patient* S2 - MH Patient Autonomy OR TI independence OR AB independence S3 - TI theory OR AB theory OR TI concept OR AB concept S1 AND S2 AND S3 |
| Database: MEDLINE (VIA PUBMED) Results: 461 Search strategy (18 de abril de 2020) (((Patients[MeSH Terms]) OR (patient*[Title/Abstract])) AND (((Independent Living[MeSH Terms]) OR (Personal Autonomy[MeSH Terms])) OR (independence[Title/Abstract]))) AND ((concept[Title/Abstract]) OR (theory[Title/Abstract])) Filters: in the last 10 years, English, Portuguese, Spanish, MEDLINE |
Source: Prepared by the authors for the present study
The relevance of articles for review was analyzed by two independent reviewers, using the title and abstract. The full articles were later retrieved after meeting the inclusion criteria. Two reviewers independently analyzed the articles in full text, intending to analyze whether they met the defined inclusion criteria. When there were differences of opinion between the two reviewers, the intervention of the third reviewer was requested. According to the study's objectives, the researchers developed an instrument with the starting point for data extraction.
The following information was mentioned for each study: a) author, year of publication and country; b) methodological design; c) characteristics of the participants; d) name of the instruments; and e) objective (s) of the study.
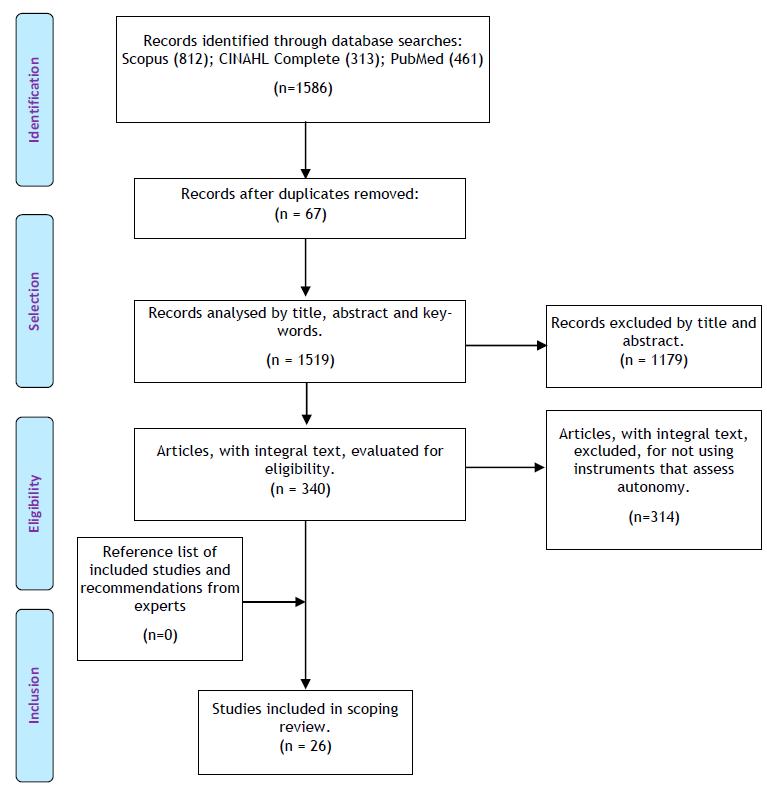
As shown in Figure 1, the survey identified 1586 articles with possible relevance for the study. Of these, 67 were extracted because they are in duplicate; of the remaining 1519 articles, 1179 articles were excluded after reading the title and abstract, 314 articles were excluded for not meeting the inclusion criteria after reading in full. After that selection, 26 articles were included.
RESULTS
Of the 26 articles that made up the sample, these are presented in table 2, including the following information: study code, authors and years, type of study, population and country, instruments used to assess independence, and study objectives or hypotheses.
Table 2 Articles under analyses, 2020
| Study ID | Type of Study | Title | Population/country | Instruments | Purpose |
|---|---|---|---|---|---|
| A1 (Anggelis et al, 2019 ) | RCT (Randomized Control Trial) | Impact of motor therapy with dynamic body-weight support on Functional Independence Measures in traumatic brain injury: An exploratory study | Patients with Traumatic Brain Injury who receive inpatient rehabilitation incorporating dynamic body weight support (DBWS) (n = 6) and who received inpatient rehabilitation without DBWS (n = 6)/USA | Functional Independence Measurement (FIM) | To determine whether the use of dynamic body weight support allows safe administration of intensive motor therapy during hospital rehabilitation and whether its use improves functional recovery more than standard therapy. |
| A2 (Chang et al., 2014) | RCT | Health Service Management Study for Stroke: A randomized Controlled Trial to Evaluate Two Models of Stroke Care | 41 patients randomized, 20 were allocated co-located acute/rehabilitation stroke care and 21 traditionally separated acute/rehabilitation stroke care/Australia | FIM | Compare the effect of two models in a randomized controlled trial on the care of stroke patients. |
| A3 (Cheville, Basford, Dos Santos, & Kroenke, 2014) | Quantitative | Symptom Burden and Comorbidities Impact the Consistency of Responses on Patient-Reported Functional Outcomes | 163 women with stage IV breast cancer and 311 adults with late-stage lung cancer/USA | FIM | To assess the influence of symptom intensity, mood and comorbidities on patient-clinical agreement and the consistency of responses to the functional results reported by the patient |
| A4 (Gerrard et al., 2013) | RCT | Validity and Reliability of the FIM Instrument in the Inpatient Burn Rehabilitation Population | 7569 subjects with burn injury/USA | FIM | Provide evidence of the validity of the MIF instrument in the person with burns in a rehabilitation program |
| A5 (Czyżewski, Szczepkowski, Domaniecki, & Dąbek, 2013) | RCT | Physiotherapy Based on PNF Concept for Elderly People After Conventional Colon Surgery | 34 patients scheduled for elective major abdominal surgery/Poland | Instrumental Activity Daily Living Scale (IADL) | Assess the functional status of the elderly after surgery during early physical therapy |
| A6 (Haines & McPhail, 2011) | Mixed study | Threat Appraisal for Harm from Falls: Insights for Development of Education - Based Intervention | 125 inpatient geriatric rehabilitation/Australia | FIM | Describe how patients perceive the threat of falls in hospitals, identify the characteristics of patients associated with greater or lesser perceptions of the threat of falls and examine whether there are differences between the risk that patients perceive in general and the risk they perceive in relation to yourself |
| A7 (Crum, Baltz, & Krause, 2019) | Case study | The use of motor learning and neural plasticity in rehabilitation for ataxic hemiparesis: A case report | 1 inpatient with stroke/USA | FIM | Describe the intervention program for a patient with ataxic hemiparesis, based on principles of motor learning and neural plasticity |
| A8 (Huseyinsinoglu, Ozdincler, & Krespi, 2012) | RCT | Bobath Concept versus constraint-induced movement therapy to improve arm functional recovery in stroke patients: a randomized controlled trial | 24 patients were randomized to constraint-induced movement therapy or Bobath Concept group/Turkey | FIM | Compare the effects of the Bobath concept and movement therapy induced by restrictions on functional recovery of the upper limb in stroke patients with high level of function on the affected side |
| A9 (Malheiro, Gaspar, & Barros, 2017) | Quantitative | Training Camp: Effects of an Educational Program For Self-management, Adolescents with Spina Bifida | 56 adolescents with spina bifida, aged 10 to18 years/USA | FIM | To evaluate a field intervention with an educational self-management program among adolescents with spina bifida |
| A10 (Ogawa et al., 2016) | RCT | Short-term effects of goal-setting focusing on the life goal concept on subjective well-being and treatment engagement in subacute inpatients: a quasi-randomized controlled trial for a randomized control trial | 66 patients in subacute rehabilitation ward/Japan | FIM | Investigate the short-term effects of the concept of life on subjective well-being and involvement with treatment and determine the sample size needed for further study |
| A11 (Pignolo et al., 2016) | RCT | A new treatment in the rehabilitation of the paretic upper limb after stroke: the ARAMIS prototype and treatment protocol | 52 patients enrolled in the study, 28 cases treated with ARAMIS and 24 controls with conventional rehabilitation/Italy | FIM | To compare the effectiveness of robotic rehabilitation by an exoskeleton prototype system with traditional rehabilitation in motor and functional recovery of the upper limb after stroke |
| A12 (Prodinger, O'Connor, Stucki, & Tennant, 2017) | Quantitative | Establishing Score Equivalence of the Functional Independence Measure Motor Scale and the Barthel Index, Utilizing the International Classification of Functioning, Disability and Health and Rasch Measurement Theory | 2414 from patients discharged from an inpatient regional rehabilitation/United Kingdom | FIM Barthel Index | Establish the equivalence between the total score of the MIF motor scale and the Barthel Index by applying the International Classification of Functionality, Disability and Health and theory of Rach measures |
| A13 (Rebagliati et al., 2016) | Quantitative | Frailty and resilience in an older population. The role of resilience during rehabilitation after orthopedic surgery in geriatric patients with multiple comorbidities | 81 orthopedic rehabilitation hospitalized/Italy | FIM | Explore the relation between resilience, fragility and quality of life in orthopedic rehabilitation and evaluate if these factors can affect the rehabilitation result |
| A14 (Saxer et al., 2018) | RCT | Minimally invasive anterior muscle-sparing versus a transgluteal approach for hemiarthroplasty in femoral neck fractures - a prospective randomized controlled trial including 190 elderly patients | 190 elderly patients/Switzerland | FIM | To evaluate the benefit of an anterior minimally invasive approach (AMIS) with a lateral Harding (LAT) approach for hemiarthroplasty in patients who are often fragile |
| A15 (Todri, Lena, & Martínez Gil, 2019) | RCT | A single blind randomized controlled trial of global postural re-education: Cognitive effects on Alzheimer disease patients | 135 patients with Alzheimer didease/Spain | Barthel Index | It is important to verify that by modifying and improving postural attitudes through GPR, a better concentration of cognitions in older people is achieved, increases self-awareness and proprioception in comparison with the effects of frequent therapies implemented in elderly centers. |
| A16 (Sharma et al., 2018) | RCT | An open-label proof-of-concept study of intrathecal autologous bone marrow mononuclear cell transplantation in intellectual disability | 58 patients with intellectual disability/India | FIM | To evaluate the safety, efficacy and clinical effects of autologous intrathecal transplantation of bone marrow mononuclear cells in a patient with intellectual disease |
| A17 (Sharma et al., 2014) | Case study | Autologous Bone Marrow Mononuclear Cells in Ischemic Cerebrovascular Accident Paves Way for Neuro restoration: A Case Report | 1 patient with Stroke/India | FIM | To observe the effects of autologous mononuclear cells in the intrathecal bone marrow on ischemic stroke |
| A18 (Singh et al., 2012) | RCT | Effects of High- Intensity Progressive Resistance Training and Targeted Multidisciplinary treatment of Frailty on Mortality and Nursing Home Admissions after Hip Fracture: A Randomized Controlled Trial | 124 patients admitted to public for repair of hip fracture/Australia | FIM Katz Índex of Activities of Daily Living (ADLs) Assessment of Living Skills and Resources (ALSAR) | Test a new evidence-based treatment strategy to improve long-term results after hip fracture, targeting sarcopenia with 12 months of high-intensity progressive resistance training |
| A19 (Richardson, Isbister, & Nicholson, 2018) | Quantitative | A Novel Treatment Protocol (Nocebo Hypothesis Cognitive Behavioural Therapy; NH-CBT) for Functional Neurological Symptom Disorder/Conversion Disorder: A Retrospective Consecutive Case Series | 13 patients with functional neurological symptom disorder/United Kingdom | FIM | It was hypothesized that FNSD arises from a belief of being neurologically damaged (via a mechanism akin to a nocebo response), and an interdisciplinary treatment protocol was developed consistent with this hypothesis, transparently sharing this theory with participants. |
| A20 (Kosteniuk et al., 2016) | Quantitative | Trajectories of Depressive Symptomatology in Rural memory Clinic Patients between Baseline Diagnosis and 1-Year Follow-Up | 144 patients diagnosed with no cognitive impairment, mild cognitive impairment, dementia due to Alzheimer’s disease, or non- Alzheimer’s disease dementia/Canada | IADL | To investigate the prevalence and trajectory of symptomatology during 1-year follow-up and the severity of depressive symptoms, by group of dementia diagnoses and determine the predictors of depressive symptoms during follow-up |
| A21 (Watabe et al., 2018) | Mixed study | Beneficial falls in stroke patients: evaluation using a mixed method design | 123 stroke patients/ Japan | FIM | To define the process by which the rehabilitation unit clinician subjectively defines a fall as a beneficial event and describes the characteristics of patients suffering from beneficial falls |
| A22 (Putcha & Tremont, 2016) | RCT | Predictors of independence in instrumental activities of daily living: Amnestic versus nonamnestic MCI | 170 patients with mild cognitive impairment/United Kingdom | IADL | To determine whether neuro-psychological measures, as well as the concept related to the patient's anosognosia, are associated with independence in daily life activities in patients with mild cognitive impairment and without any cognitive impairment |
| A23 (Klietz et al., 2018) | Quantitative | Impaired Quality of Life and Need for Palliative Care in a German Cohort of Advanced Parkinson´s Disease Patients | 76 geriatrics patients with advanced idiopathic Parkinson’s disease/Germany | Barthel Index | To investigate the current status of the implementation of palliative care and quality of life in a local cohort of patients with advanced Parkinson's disease, in order to structure and improve future care |
| A24 (Yang & Lee, 2015) | Quantitative | Analysis of the medical demands of elderly dementia patients conserving the caregiver cost of medical accompaniment: an application of the travel cost method and altruistic utility function | 201 dependent older adults with a risk of developing Alzheimer’s disease/Taiwan | Barthel Index | Establish an outpatient medical demand model for visits to elderly people with dementia and their caregivers |
| A25 (Tyson, Burton, & McGovern, 2015) | Quantitative | The effect of a structured model for stroke rehabilitation multidisciplinary team meetings on functional recovery and productivity: a Phase I/II proof of concept study | 36 inpatients stroke rehabilitation/United Kingdom | Barthel Index | Evaluate the feasibility, acceptability and impact of the model to structure multidisciplinary team meetings, their implementation in compliance with the quality and results of patients |
| A26 (Van Der Zee, Visser-Meily, Lindeman, Kappelle, & Post, 2013) | Quantitative | Participation in the Chronic Phase of Stroke | 111 patients with Stroke/Netherlands | Utrecht Scale for Evaluation of Rehabilitation (USER) | To describe the participation (objective and subjective) and determine how physical and cognitive independence and subjective complaints (pain, fatigue and mood) influence participation in community-based stroke survivors in the Netherlands |
Source: Prepared by the authors for the present study
The articles were categorized according to the methodology used in the study, with ten quantitative studies, twelve experimental studies, two mixed studies, and two case studies. Five of these studies were carried out in the USA, three in Australia, four in the United Kingdom, two in Japan, two in Italy, two in India, one in Canada, one in Poland, one in Turkey, one in Switzerland, one in Spain, one in Taiwan, Netherlands and Germany.
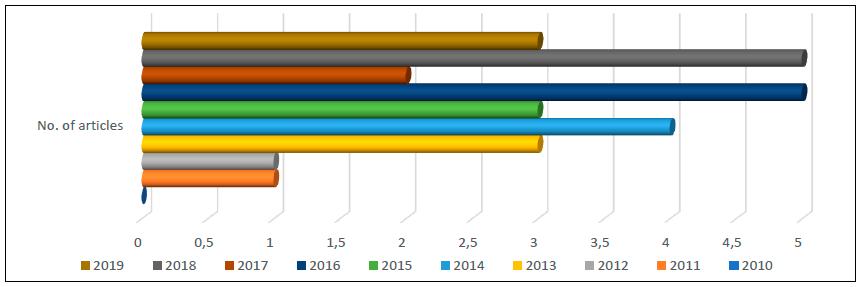
As for the year of publication, in figure 2, we observe the distribution by year of publication, highlighting that the research was restricted to the period between 2010 and 2020 and that in the ten years included in the research, the years 2016 and 2018 stand out with five articles each.
Source: Prepared by the authors for the present study
Figure 2 Distribution of studies, according to the year of publication, 2020.
In a total of 26 publications, it was possible to identify six different instruments, namely: Functional Independence Measurement (FIM) (n = 18), Instrumental Activities of Daily Living Scale (IADL) or Lawton-Brody Index (n = 3), Barthel Index (n = 5), Katz Index of Activities of Daily Living (ADLs) (n = 1), Assessment of Living Skills and Resources (ALSAR) (n = 1) and Utrecht Scale for Evaluation of Rehabilitation (USER) (n = 1). Two of the studies selected in the survey used more than one instrument to assess independence.
The FIM is a scale that evaluates the patient’s performance in executing a set of 18 tasks. Motor assessment includes the sub-scales: self-care, which is divided into 6 items, toilet control has two items; mobility has 3 items and locomotion, has 2 items. The cognitive assessment of the scale includes the sub-scales: communication with 2 items and social cognition with 3 items. Of the 18 items, 13 assess motor functions and 5 assess cognitive functions. The score for each item varies from 1 to 7, according to the degree of dependence: 7 corresponds to complete independence, 6 to modified independence, 5 to the need for supervision while performing the task, 4 to minimal help, that is, the patient makes 75% of the effort required in the task, 3 to moderate help, with the patient performs 50% of the effort needed to complete the task, 2 maximum help, where the patient performs more than 25% of the task, 1 full help, that is, the patient has to be replaced for the entire task . In the present study, this instrument stands out, as it was used in 18 of the 26 selected studies .
In the IADL, the person’s level of independence is assessed concerning performing instrumental activities that comprise eight tasks such as the ability to use the telephone, shopping, food preparation, housekeeping, laundry, mode of transportation, responsibility for own medications, and ability to handle finances. This instrument is scored from 0 to 8, where 0 is dependent, and 8 is independent 34. This instrument was used in three of the selected studies .
Barthel Index assesses the patient’s level of independence to perform ten activities of daily living such as eating, personal hygiene, using the toilet, bathing, dressing and undressing, sphincter control, walking, transferring from the chair to the bed, up and downstairs. The minimum score is zero and corresponds to the maximum dependency and 100, corresponds to the maximum score, and is equivalent to a state of independence total for the daily activities of life evaluated. Therefore, on this scale the total can vary from zero to 100, and when the total is between zero and 20, the person has total dependence, between 21 and 60, it is considered a serious dependency, 61 and 90, a moderate dependency, 91 and 99, a very light dependency and 100, is an independent person 38. This tool was used in five studies of the selected studies (25, 39-43).
The ADLs is an appropriate instrument for assessing functional status and serving as a measure of the patient’s ability to carry out activities of daily living independently. The scale classifies performance adequacy into six functions: bathing, going to the bathroom, transferring, continence, mobility, dressing/undressing, and feeding. Patients are classified, whether yes or no, for independence in each of the six functions. A score of six indicates the complete function, 4 indicates moderate impairment and 2 or less indicates severe impairment or very dependent 44. Of the selected studies, this tool was only used by one study 30.
ALSAR is a tool that allows to systematically assess the performance of 11 tasks of daily living, classifying the patient’s skill levels and resources separately for each task, and combining these levels to determine the risk. These tasks include skills and resources for telephoning, reading, leisure, medication management, money management, transportation, shopping, meal preparation, laundering, housekeeping, and home maintenance. For each task, skills are scored: 0 for independent and consistent performance, 1 for partial performance, and 2 for non-responsibility for the task. For the total of the scale, results between zero and 22 points can be obtained. The resources are scored: 0 for adequate to perform the task consistently, 1 for partially supporting the task, or 2 for insufficient for the task or available resources are not being used. For their application, the authors suggest some questions that facilitated the correct data collection 45. This instrument was used only by one of the selected studies 30.
The USER is a scale that assesses physical and cognitive independence and subjective complaints. This scale allows the evaluation of three dimensions of participation: frequency (objective perspective), restrictions (subjective perspective), and satisfaction (subjective perspective). The physical independence subscale consists of 14 items on mobility and self-care. The Cognitive Independence subscale consists of 10 communication, applied cognition, and behaviour items. All items are scored on a six-point scale, from zero (<50% independent) to five (independent without difficulty and assistance or adaptation), with higher scores reflecting more independence. Subjective complaints consist of pain (1 item), fatigue (1 item), and mood (4 items: depressed mood, sadness, anxiety, and anger), all rated on a scale from zero (nothing) to 100 (worse), with higher scores reflecting more subjective complaints (46,47). As for the last two instruments, this one was also used only by one of the selected studies 47.
DISCUSSION
The use of scales to assess people’s needs has increased over time, as has the construction of new tools, as these allow professionals to target the needs of care and at the same time realize the gains in health, with the implementation of specific therapies and intervention programs, thus allowing to reinforce the importance, for health care 48.
According to the analysis of the concept of independence carried out, an independent person is someone capable of self-care and carrying out daily life activities, both basic life interventions (self-care, mobility, food, personal hygiene, using the toilet, dressing, undressing and putting on shoes), as well as instrumental interventions of daily living (going shopping, managing money, using the phone, cleaning, cooking, use transportation), without the help of third parties 5. Taking into account this analysis, it can be seen that most instruments or assess self-care, also called basic activities of daily living (30,39) or instrumental activities of daily living (30,36), therefore, no instrument evaluates independence in its essence, as they not evaluate the two aspects together.
The FIM and USER scales also address the cognitive domain, which is essential for an autonomous life (15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 31 32 33 35 36 37,47). According to the analysis of the concept of autonomy, it comprises the physical domain, the cognitive domain, the social domain, and the management of emotions 6. Considering that these two instruments are used in the area of rehabilitation, the need for them to also understand the cognitive domain is justified, as this can influence health gains in the physical domain and vice versa 49. However, when analyzing the description of the instruments, the authors refer to independence. It can also be inferred that there may be some confusion in the definition of both concepts when it is intended to assess independence and includes aspects that are understood by the concept of autonomy, since in the different areas of knowledge, there is some confusion between autonomy and independence. In clinical practice, in the health area, the term independence is regularly seen when it is intended to promote autonomy and vice versa.
Suppose the professional, namely the nurse, intends to assess autonomy, in the true essence of the concept. In that case, they should use concomitantly other instruments besides those mentioned, because only then will they be able to measure what they want. In addition to the instruments described, some intend to measure autonomy such as: The Health Care Climate Questionnaire, Treatment Self-Regulation Scale, Basic Needs Satisfaction in General Scale, Impact Participation and Autonomy, Autonomy Preference Index and the Perceived Parental Autonomy Support Scale, for example. However, these instruments must be translated and validated for the Portuguese population.
Maintaining activities of daily living simultaneously favours the cognitive state; thus, motor and social stimulation are fundamental to preserve autonomy in daily activities 50. Thus, it is possible to understand the importance of physical and also cognitive rehabilitation, justifying the disciplinary intervention, in nursing, of the specializations of rehabilitation nursing and mental health and psychiatry 46,47. Through the implementation of rehabilitation programs, these professionals have demonstrated their effectiveness in the physical, cognitive, psychological, and even social recovery (49,50).
The person’s cognitive decline may be associated with a specific pattern of functional losses in all activities of daily living, first of all, advanced activities of daily living, followed by instrumental activities of daily living and finally basic activities of living daily 50.
USER also allows the assessment of subjective complaints, which are also essential components in the rehabilitation process, both in the acquisition of physical and cognitive skills. The person's cognitive decline may be associated with a specific pattern of functional losses in all activities of daily living, first of all advanced activities of daily living, followed by instrumental activities of daily living and finally basic activities of living daily or also known as self-care 50. Humor is part of the emotional management capacity, which is part of the concept of autonomy and not that of independence. Although the importance of this is understood for the promotion of independence, through the rehabilitation programs, since this promotion necessarily depends on the person's motivation, it does not measure independence, but rather autonomy.
Therefore, it is suggested that the title of the instruments and their description reflect the evaluated components, that is, the basic activities of daily living, and/or instrumental activities of daily living, both considered in the concept of independence. Health professionals, and in particular nurses, due to their proximity to the patient and their family, must be able to provide appropriate responses to their real needs, being necessary for this, the knowledge of the tools at their disposal and the use of the concepts, which are proper to them 8. When the application of the different instruments is combined, together they can respond to the concept of independence, which is why its implementation is recommended.
The assessment instruments implemented in clinical practice thus constitute essential tools that collaborate in identifying real or potential problems of the person being cared for. Hence, their correct application is essential, so that the definition of this same problem is correctly systematized thus contributing, for the prescription of necessary nursing interventions. Only with a thorough knowledge of these components, each professional can reflect and examine their practices and be able to maintain or modify their performance.
Although the time limit of 10 years was chosen to obtain the most recent evidence, this is still a limitation of the present study. Also, it would be interesting to increase the search in more databases, which is another limitation of the present study. A limitation of the studies included in this scoping is the confusion between autonomy and independence concepts, which we tried to clarify.
CONCLUSION
The present study sought to map the instruments to assess independence, using a scoping review, noting that the most used instrument is the FIM and then the Barthel index, the IADL, the Katz Index of Activities of Daily Living. ALSAR and USER, in the selected studies, were the least used.
Since there are no measurements/evaluations, as there is no instrument that assesses only, or in isolation, independence, the quality of care provided and its gains in this dimension become difficult to measure.
Scientific evidence recognizes the relationship between the quality of care provided and the application of instruments capable of measuring health gains. The assessment instruments are thus considered essential tools for the practice of care. These allow professionals to know the health status of the people they care for, combined with clinical evaluation, and direct care, according to the person's real or potential needs. Being the nurse, the professional who gathers skills to promote independence, it is up to this professional to know in detail the tools they have available to carry out this assessment. The importance of independence for the quality of life that the person experiences is recognized. In this way, these professionals could contribute to obtaining health gains and, consequently, promoting the health of populations.

