











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
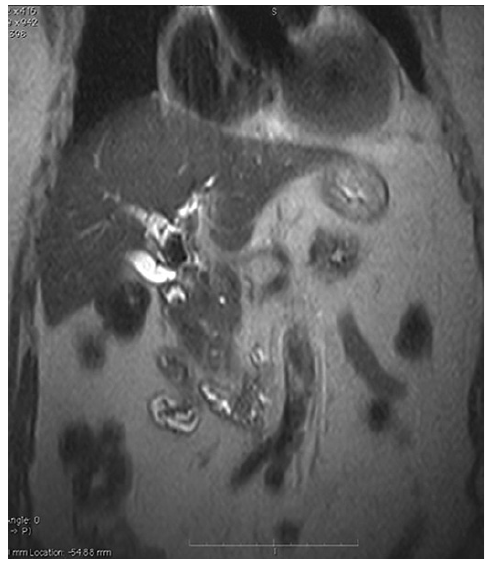
PermalinkEighty-Seven-year-old woman, without relevant medical past history, was referred to ERCP for treatment of acute cholangitis. Abdominal CT scan revealed dilatation of intra and extrahepatic bile ducts with hyperdense content in the cystic duct and in the common bile duct, suggestive of Mirizzi syndrome and choledocholithiasis. An abdominal MRI was performed revealing a large 4 cm stone in the infundibulum-cystic duct, a 2 cm stone in the hepatic duct (Fig. 1).
During the initial ERCP, cholangiography revealed a large stone in the cystic causing a stenosis of the hepatic duct with upstream dilation of the biliary tree, confirming the Mirizzi syndrome (Fig. 2). A plastic double pigtail stent (7 Fr × 4 cm) was inserted, after sphincterotomy. After multidisciplinary evaluation of the patient conditions, given the patient frailty it was decided to treat the condition using an endoscopic approach - laser lithotripsy assisted by cholangioscopy.

SpyGlass cholangioscopy revealed two impacted large stones, one in the cystic duct and unexpectedly, another in the hepatic duct. Lithotripsy with laser Holmium was successfully performed in both stones; after both lithotripsies, a fistula between the cystic and the hepatic duct was noticed, involving less than one-third of the circumference of the hepatic duct (Mirizzi type II). The patient presented a favourable clinical evolution and was discharged 4 days after the procedure.
Discussion
Mirizzi syndrome is an uncommon cause of acute cholangitis [1]. ERCP allows the resolution of jaundice through the placement of stents and, in some cases, the removal of the cystic duct stone, although most patients are treated surgically [1-3]. The use of cholangioscopy-guided lithotripsy with the Spyglass platform was already described in the treatment of patients with Mirizzi syndrome in some case reports [3-5].

