











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Nonsuicidal self-injuries (NSSIs; e.g., cutting, burning, and biting) are characterized as acts of destruction of one’s body tissue with a direct and intentional nature, distinct from culturally sanctioned acts and without suicidal intent (Nock, 2009, 2010). In college students, the prevalence of NSSI varies from 20.2% (cf. Swannell et al., 2014) to 38.9% (Cipriano et al., 2017). From a functional perspective, NSSI most commonly serves the function of emotion/affective regulation (Cipriano et al., 2017), especially the elimination/avoidance of negative emotions (Klonsky, 2007). According to Nock and Prinstein’s model (2004), NSSI can serve four major functions, namely intrapersonal-negative reinforcement (e.g., to decrease/distract from negative thoughts/feelings), (b) intrapersonal-positive reinforcement (e.g., to generate feelings/sensations when experiencing numbness or anhedonia), (c) interpersonal-negative reinforcement (e.g., to escape from some undesirable social situation), or (d) interpersonal-positive reinforcement (e.g., to communicate with/seek help from others). Therefore, NSSI seems to be related to emotion dysregulation (Hasking & Claes, 2020; Miller & Racine, 2020). In a study conducted by Guérin-Marion and colleagues (2020), the authors found that students with recent NSSI had greater emotion dysregulation than peers with past NSSI, both groups of students evidencing greater emotion dysregulation than the ones without past NSSI.
Previous research has also shown that NSSI is associated with depressive symptomatology (Silva et al., 2017; Taliaferro & Muehlenkamp, 2015). In fact, college students with NSSI in the past year were more depressed than peers without current NSSI and those which NSSI occurred more than a year ago (Saraff & Pepper, 2014; Smith et al., 2015). However, less is known about the relationship between NSSI and self-criticism (Zelkowitz & Cole, 2020). Considering the main conclusions of two studies, students with past NSSI reported greater self-criticism than peers without NSSI lifetime (Hamza et al., 2014) and students with NSSI in the past year reported greater levels of self-disgust than those with NSSI for more than a year ago (Smith et al., 2015).
Considering the association between emotion regulation, depressive symptomatology and self-criticism, previous research with college students postulated that emotion dysregulation and self-criticism are often related to depressive symptomatology and may interact over time in the development and maintenance of depressive symptomatology (Werner et al., 2019). Additionally, both emotion dysregulation and self-criticism seem to be common in college students with NSSI. In fact, Kranzler et al. (2016) showed that emotion dysregulation increased the probability of college students developing internalizing symptoms, leading to the use of NSSI to reduce distress and negative emotions. Accordingly, Smith et al. (2015) showed that self-criticism, more specifically self-disgust, mediated the relationship between depressive symptomatology and NSSI. On the other hand, NSSI may serve the function of emotion regulation, allowing the individual to eliminate or avoid negative emotions and, in turn, depression can be associated with emotion avoidance, achieved through NSSI. Despite the well-known associations between these variables, few is known about the mechanisms under which these variables seem to be related in past and current NSSI. Therefore, this study aimed to (1) evaluate the frequency of lifetime and current NSSI (2) compare college students without NSSI, with past NSSI and with current NSSI regarding depressive symptomatology, emotion dysregulation, and self-criticism; and (3) analyse the mechanism under which self-criticism, depression, and emotion regulation may affect each other and whether this mechanism is structurally different between the three groups.
Method
Participants
The participants were 385 college students (85.2% females) between 18 and 35 years old (M=20.71; SD=2.80) from three Portuguese Universities. The majority of the participants (94.3%) reported having Portuguese nationality and 98.7% were single. According to the parents’ academic qualifications, most of the participants (50.8%) were in middle socioeconomic level; 38% were in high socioeconomic level and 11.3% in middle-low socioeconomic level.
Measures
Difficulties in Emotion Regulation Scale - Short-Form (DERS-SF; Kaufman et al., 2016; Portuguese version by Moreira et al., 2020). This self-report questionnaire assesses the difficulties in emotion regulation, consisting of 18 items into six subscales. The subscales, correspond to difficulties in different dimensions of emotion regulation: Nonacceptance (α=.88) (e.g., when I´m upset, I become embarrassed for feeling that way”), Goals (α=.91) (e.g., “when I’m upset, I have difficulty getting work alone”), Impulses (α=.92) (e.g., “when I’m upset, I become out of control”), Awareness (α=.70) (e.g., “I pay attention to how I feel”), Strategies (α=.82), (e.g., “when I’m upset, it takes me a long time to feel better”), and Clarity (α=.81) (e.g., “I have no idea how I am feeling”). The DERS-SF revealed good internal consistency in this study for all the subscales and total scores (α=.92).
Depression Subscale of the Depression, Anxiety and Stress Scale (DASS-21; Lovibond & Lovibond, 1995; Portuguese version by Pais-Ribeiro et al., 2004). Given the study’s objectives, only the depression subscale (e.g., “I couldn’t seem to experience any positive feeling at all”) of the DASS-21 was used, covering the concepts of dysphoria, discouragement, devaluation of life, self-depreciation, lack of interest/involvement, anhedonia, and inertia. In this study, the depression subscale presented a high internal consistency (α=.93).
The Inadequate Self and Hated Self Scales of the Forms of Self-Criticizing and Reassuring Scale (FSCRS; Gilbert et al., 2004; Portuguese version by Castilho & Gouveia, 2011). This self-report consists of 22 items to examine how critical/attacking or how supportive/reassuring people are when things go wrong with them (e.g., “when things go wrong for me, there is a part of me that puts me down”). Items are organized into three subscales: Inadequate self, Hated self, and Reassuring self. Considering the aims of the present study, only the subscales inadequate self and hated self were used. In this study, a high internal consistency was evidenced for the inadequate self (α=.93) and hated self (α=.87) subscales, as well as for the total scale of self-criticism (α=.94).
Self-Injury Questionnaire - Treatment Related - Short-Form (SIQ-TR-SF; Claes & Vandereycken, 2007; translated by Gonçalves, 2007). This self-report questionnaire of 12 items assesses past and current NSSI. First, the participant is asked if he or she has ever been involved in NSSI, with no intention of killing oneself, and if the answer is affirmative, the following items assess the typology(s) of injury(s) and how long ago the behaviour(s) was performed. The NSSI functions were scored on a scale ranging from 1 (not at all) to 5 (very much). The items are distributed across four scales, according to the four-function Nock and Prinstein’s model (2004): automatic-negative reinforcement (e.g., “to avoid or suppress negative feelings”), automatic-positive reinforcement (e.g., “to feel something, even if it was pain”), social-negative reinforcement (e.g., “to avoid school, work, or other activities”) and social-positive reinforcement (e.g., “to feel some pleasure”). SIQ-TR-SF allows the assessment of five types of NSSI: scratching, bruising, cutting, burning, and biting oneself; additionally, the subject can specify another type of NSSI.
Procedure
Data were collected from Portuguese universities, both public and private, between December 2020 to March 2021. As inclusion criteria, age between 18 and 35 years old and Portuguese as a native language were considered. The data were collected online through the Google Forms platform. Social networks were used to publicize the study, in which participation was requested and the link was shared and directed participants to the Google Forms platform, to complete the battery of measures. For Psychology students at the University of Minho, the study protocol was made available in the Crediting System of the School of Psychology at the University of Minho, where the link that conducted the participants to the Google Forms platform was presented.
The study was approved by the Ethical Committee of the University and participants provided written informed consent prior to study-related procedures.
Statistical analyses
All statistical analyses were performed using the R statistical environment (Rstudio, version 3.6.2, R Core Team, 2019) with the “lavaan” package (Rosseel, 2012). Items composing scales and subscales were averaged, and these means were included as single variables in the dataset. Between-group differences were assessed for all sociodemographic and clinical variables. Then, a multigroup mediation model was evaluated using structural equation modelling (SEM) statistical tools. Bootstrap standard errors were computed (see Appendix 1).
Results
Of the 385 participants, 90 (23.4%) reported lifetime NSSI (more specifically, 16.4% reported NSSI more than a year ago and 7% reported NSSI in the current year), and 295 (76.6%) reported no NSSI. Of the 90 participants with NSSI, 20 (22.2%) reported only a single NSSI method, whereas 70 (77.8%) reported two or more methods, with “cutting” being the most reported. In addition, 69 (76.7%) participants indicated NSSI on their “arms, hands, fingers, and nails”. Likewise, 76 (84.4%) participants reported NSSI “1 to 5 days” per month. Also, 66 participants (73.3%) reported had hidden the NSSI from other people. In addition, 54 (60%) participants reported that NSSI was not clearly planned ahead and 27 (30%) reported “never” caring for the wounds. Moreover, 68 (75.6%) participants reported to feeling pain from “sometimes” to “often” and 79 (87.8%) feeling “little” to “moderate” pain.
There was no statistically significant association between gender and NSSI, χ2 (1,N=385)=1.27, p=.260. Also, no statistically significant correlation was found between age and NSSI, rpb(383)=-.05, p=.317.
Differences between groups in depression symptoms, emotion regulation, and self-criticism
Statistically significant differences were observed between the non-NSSI group vs. past-NSSI group, between the non-NSSI group vs. current-NSSI group, and between the past-NSSI group vs. current-NSSI group. Thus, the non-NSSI group had a lower score on the depression subscale than the other two groups. Statistically significant differences were also observed between the groups regarding emotion regulation. Specifically, there were significant differences between the non-NSSI group vs. the past-NSSI group and the non-NSSI group vs. the current-NSSI group on the DERS total scale. Subsequently, statistically significant differences were evidenced between the non-NSSI group and the current-NSSI group in the subscales Clarity, Goals, Strategies and Non-Acceptance. The current-NSSI group reported higher scores on these subscales than the non-NSSI group. Significant differences were also found between the non-NSSI group vs. past-NSSI group in the in the subscales Clarity, Impulses and Strategies. The past-NSSI group reported higher total scores on these subscales than the non-NSSI group. Finally, significant differences were found in the Goal’s subscale scores between the past-NSSI group and the current-NSSI group, with the current-NSSI group reporting higher scores. Regarding self-criticism, statistically significant differences were evidenced between the groups in the total score and in the subscales of the FSCRS (Table 1). The non-NSSI group had lower scores on the total score and in the Inadequate Self and Hated Self subscales compared to both NSSI groups. Additionally, the current-NSSI reported higher scores when compared to the past-NSSI group in these three subscales.
Table 1 Comparison between groups
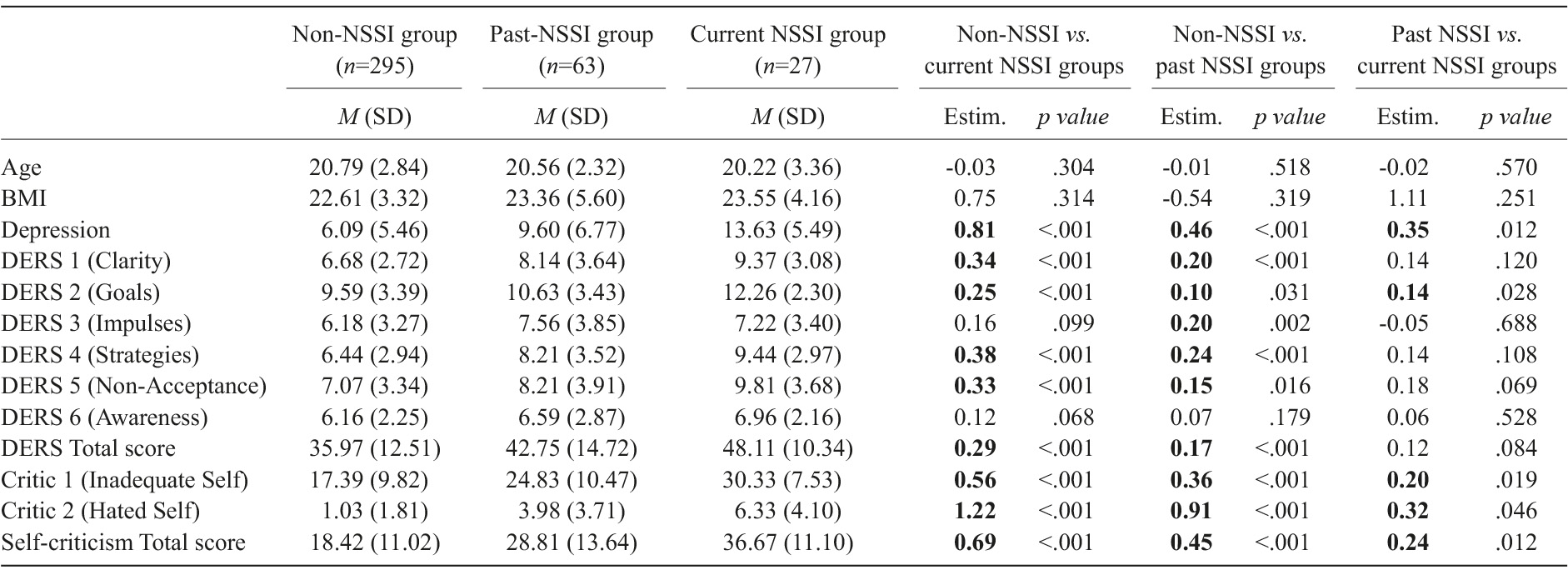
Note. Bold values highlight significant differences (p<.05). Abbreviations: BMI - Body Mass Index; DERS - Difficulties in Emotion Regulation Scale; Estim. - Estimate. Group differences were estimated using regression modelling with appropriate distribution families (the Conway-Maxwell-Poisson family for positive integer data and robust regression for BMI).
Mediation model
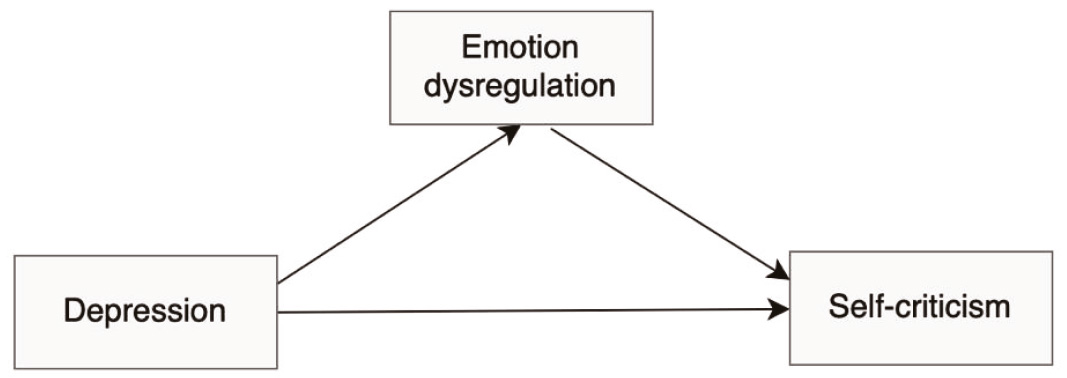
To understand the mechanism under which self-criticism, depression, and emotion regulation affect each other and whether this mechanism is structurally different between the three groups, all (six) possible mediation models between those variables were assessed for each group independently in a multigroup mediation analysis. Among all these mediation models, there was only one that showed a significant mediation effect for all groups simultaneously, suggesting that it represents the strongest interplay mechanism between these three variables in general. This model is outlined in Figure 1 and presents emotion regulation as a mediator in the relationship between depression and self-criticism. In fact, for the current-NSSI group, this was the only model that had a significant mediation effect.
The results of the multigroup mediation model are summarized in Figure 2. It is shown that, in all groups, higher levels of depression are associated with higher levels of emotion dysregulation, which in turn are associated with higher levels of self-criticism. Although the coefficients of the multigroup mediation model suggested structural differences between the three groups, further SEM analyses were conducted to evaluate the possible appropriateness of a single-group moderated mediation model. To check the invariance of structural paths and of residual variances (Ryu & Cheong, 2017), the multigroup model was compared to the model with equal regression coefficients and residual variances. However, significantly different (p=.0217) model fits confirmed the moderating role of the group and the adequacy of the multigroup mediation model depicted in Figure 2 to compare the indirect effects between groups.
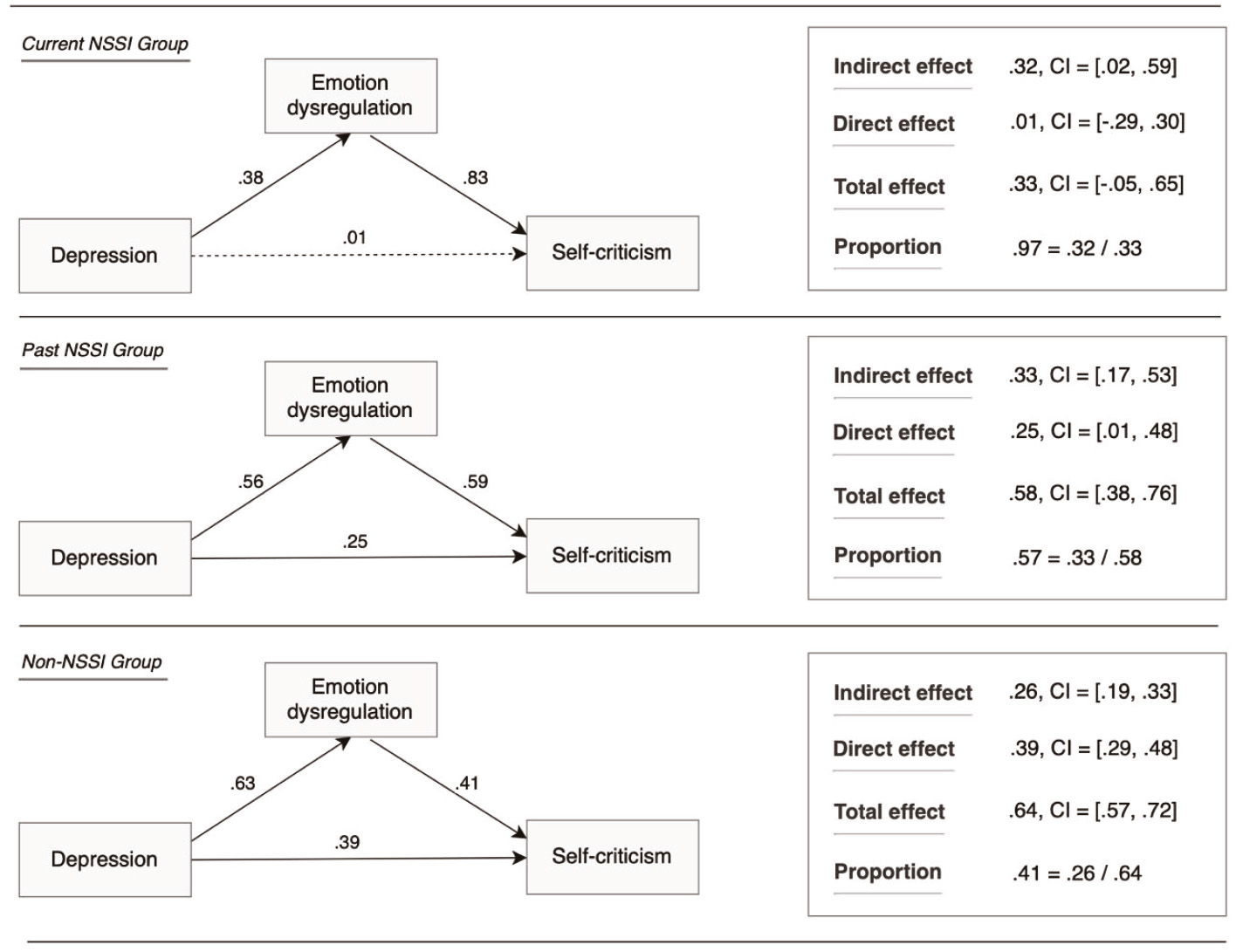
Although this model shows that the mediation of emotion regulation is established for the three groups, there are some important between-group differences (moderation) that must be acknowledged.
In the current-NSSI group, the proportion of the mediated effect is high (.97=.32/.33). Indeed, after controlling emotional regulation, the direct effect of depression on self-criticism is negligible (estimate=.01, 95%, CI [-.29.30]), i.e., it is highly nonsignificant. For this reason, this is called a “complete mediation”. Moreover, the total effect of depression on self-criticism only approaches significance (estimate=33, 95%, CI [-.05.65]), a fact that emphasizes the importance of considering emotion regulation as a key construct to understand how depression symptoms increase self-criticism in NSSI.
In the other two groups, as NSSI decreases, the direct and the total effects of depression on self-criticism become stronger, and the proportion of mediation effect becomes weaker. This means that, in addition to the indirect effect mediated by emotion regulation, there is a different path for these two groups under which depression affects self-criticism, especially for the non-NSSI group. Hence, in the non-NSSI and past-NSSI groups, higher depression can increase self-criticism without impairing emotional regulation, a fact that is not observed in the current-NSSI group.
Discussion
Almost one quarter of the college students reported NSSI at some point in their lives. This prevalence falls within the ranges reported in previous studies with college students (e.g., Lewis et al., 2019; Vega et al., 2018), however in the present study, NSSI was higher than the one reported in previous studies also conducted with Portuguese college students (e.g., Braga & Gonçalves, 2014; Silva et al., 2017). The fact that data were collect post COVID-19 lockdown, may explain this increase in the reported NSSI frequency. However, more studies are needed to evaluate the impact of COVID-19 lockdown on the NSSI development. Furthermore, as hypothesized and evidenced in previous studies conducted with college samples (e.g., Jacobson et al., 2015), students with lifetime NSSI reported higher depressive symptomatology than peers without NSSI. It is possible that there may be some vulnerability underlying depressive symptomatology (Liu et al., 2019). However, in other studies, this difference between students with past NSSI and without NSSI has not been observed in depressive symptomatology (Smith et al., 2015). It would be useful for future studies to help shed light on the depressive symptomatology maintenance towards NSSI interruption. As Burke et al. (2019) demonstrated, NSSI in adults predicted depressive symptomatology over six months (but not over shorter periods).
Students without NSSI showed less emotional dysregulation than those with past and current NSSI. Specific dimensions of emotion dysregulation stood out, particularly access to effective emotion regulation strategies, in which college students with past NSSI showed greater emotion regulation difficulties. With this limitation in self-regulatory strategies, students may use ineffective strategies to deal with negative emotions, eventually using NSSI, which effectively reduces these emotions and may reinforce NSSI development, making it not worth considering learning from other effective and adaptive emotion regulation strategies. Once students with past NSSI reported greater emotional dysregulation than those without NSSI, emotional regulation difficulties seem to remain, regardless of NSSI interruption. Contrary to expectations, students with current and past NSSI experience did not differ in emotion dysregulation, so difficulties in emotion regulation appear to remain despite NSSI interruption in the past year. It would be interesting to assess whether students with past NSSI are currently using other ineffective strategies of emotion regulation (e.g., alcohol consumption). Future studies should assess and explore different pathways related to emotion dysregulation and NSSI.
Students without NSSI also demonstrated lower self-criticism than those with current and past NSSI; among these, students with current NSSI showed higher self-criticism. Accordingly, self-criticism appears to be an important factor in NSSI development and maintenance (Nock, 2009). More specifically, the destructive component of self-criticism was the one that differed between students with past and current NSSI, seeming to be important for NSSI perpetuation, which come across as consistent given the possible anger and desire to assault the self when facing situations of perceived failure and error. The greater self-criticism found in students with past NSSI may explain why 80% of them reported using NSSI as self-punishment (Hamza et al., 2014). Once students with current NSSI were found to be the most self-critical, self-criticism may also represent a consequence of current NSSI. Effectively, in recent studies, NSSI predicts self-criticism at 12 months but not at one and six months later (Burke et al., 2019). Again, ascertaining this question would help to understand the pathways that may be related to NSSI development and maintenance.
Emotion regulation mediated the relationship between depression and self-criticism, but only for the participants with current NSSI. We may conclude that emotional dysregulation affects the strength/direction of this relationship, also in accordance with Nock’s model (2009). Accordingly, emotional dysregulation and a more general NSSI vulnerability, both, may interact with self-criticism, a specific factor of these behaviors. Additionally, the affective dysregulation underlying depression seems to explain the relationship between depression and NSSI, possibly explaining the potential interplay between emotional dysregulation and depressive symptomatology. The pathway that sustains the association between NSSI, depressive symptomatology, emotion dysregulation and self-criticism is now clearer. Therefore, we can conclude that emotion regulation mediates the relationship between depressive symptomatology and self-criticism in college students with current NSSI.
This study contributes to the understanding of the impact and interplay of depressive symptomatology, emotional dysregulation, and self-criticism on NSSI in college students, which had not yet been explored. The high NSSI frequency highlight the importance of continuing to investigate this public health problem in college populations, including in Portugal, where studies are scarcer.
Some limitations should be pointed out. First, the cross-sectional design and second, the convenience and not heterogeneous sample.

