











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
The aging process encompasses changes that affect the components of the musculoskeletal and osteoarticular function, causing declines that have a direct impact on the ability to perform routine activities, with consequences on health and physical functionality, associated with the independence and autonomy of the elderly person (Dias, 2009). Many of these conditions are accompanied by pain and, in a significant portion of them, chronic pain is the main complaint. This fact can significantly affect the quality of life of the elderly. In the context of locomotor system disorders, pain is the most frequent symptom and one of the main causes for seeking medical assistance (Kayser et al., 2014).
This change in the Brazilian age structure is directly related to the epidemiological transition, because, as the population ages, the prevalence of chronic health problems increases. Among the consequences that demographic transition and longevity bring to society, pain is one of the most significant. In many cases, chronic pain is the main complaint of individuals, interfering considerably in the quality of life of the elderly (Dellaroza et al., 2007).
Pain is understood as a multifactorial phenomenon composed by tissue damage and emotional, socio-cultural and environmental aspects. The International Association for the Study of Pain (IASP) has defined it as an emotional, sensitive, unpleasant experience lasting more than three months. It is one of the most important health problems that interfere with the performance and autonomy of the elderly in their daily life functions. Functional independence is a fundamental factor for the health of the elderly. When dependence is present, at any level, their well-being and quality of life are affected (Cunha & Mayrink, 2011).
The repercussions of chronic pain on the quality of life of the elderly population are also associated with depression, changes in family dynamics, social withdrawal, a higher prevalence of falls, cognitive dysfunction, emotional and sleep disorders and others. The high prevalence of chronic pain demands the use of greater financial and health resources, which reflects negatively on health systems, the individual and society (Araujo et al., 2010; Cunha & Mayrink, 2011).
Given this scenario, there are different ways of aging and, mainly, different ways of looking at old age. However, in history, the perception of old age associated with wear, losses and diseases is frequent. Lately, this correlation has been questioned, since several experiences of successful aging have been portrayed, for example, in social groups. The representation of old age is a concept that adheres to the identity of the elderly as subjects of society and in their own perception as a group (Daniel et al., 2015). According to Baltes and Smith (2003), successful aging strategies result from a dynamic psychosocial construct, whose expression reaches its peak in adulthood, accentuating in aging. This construct is characterized by a selection and compensation plan with specific personal and contextual characteristics. Its focus is the continuous search for an effective way to deal with losses through psychological strategies, allocating internal and concrete resources and approaching an adaptive development theory.
Successful aging is revealed in elderly people who maintain autonomy, independence and active involvement with personal life, family, friends, leisure and social life. It is revealed in productivity and in the preservation of adult partner roles. It translates into self-descriptions of satisfaction and adjustment. It is reflected on social recognition. People contribute to society or family groups, allowing them to be seen as models of successful aging (Neri & Yassuda, 2012). Maintaining the quality of life and autonomy of the elderly minimizes the occurrence of illnesses and impairments in physical, psychological and social functionalities. One way to quantify the quality of life is to associate it with the degree of autonomy in which the elderly person performs their functions in their daily lives. Such autonomy makes them independent within a social, economic and cultural context. Quality of life in old age is not an attribute of individual responsibility, but a product of the interaction between people living in a changing society (Neri, 2011).
However, changes in habits of the elderly population have been observed, with an increase in physical activities, aiming to reduce the appearance and worsening of the comorbidities inherent to this age group. Given these characteristics, active aging allows people to realize their potential for physical, social and mental well-being throughout life. It also aims to allow their participation in society according to their needs, desires and capabilities, in order to develop opportunities for health, participation and safety, to improve the quality of life as people get older (Safons et al., 2018).
Based on this context, the objective of this study is to analyze the association of osteoarticular and musculoskeletal disorders (OMD) and chronic pain (CP) with successful aging, quality of life (QOL), body mass index (BMI), physical activity level (PAL) and length of time practicing water aerobics.
Method
The present study has a quantitative, descriptive and cross-sectional design.
Participants
The population of this study was composed of elderly people who participate in the water aerobics project. Their participation in the water aerobics project occurs weekly, over a pre-established period of 8 months. The sample in this study was non-probabilistic for convenience and comprised 101 Brazilian participants of both genders, over the age of 60, consisting of elderly people who regularly participate in the water aerobics activities. The inclusion criteria established were to be over 60 years of age, not to be institutionalized or hospitalized, to have mental and health conditions to have independence and autonomy to participate in the study and sign the Informed Consent Form. The exclusion criteria determined by the research were to present dementia, frailty syndrome, to be hospitalized or institutionalized.
Material
The data collection instruments used in this study refer to sociodemographic variables and the presence of musculoskeletal and osteoarticular disorders, pain assessment (Multidimensional Pain Assessment Scale), quality of life (EUROHISQOL), successful aging (SOC), body weight status and physical activity level (IPAQ - adapted long version).
Multidimensional pain assessment scale. This scale evaluates the painful experience considering its multidimensionality, complexity and subjectivity. On the pain intensity scale, 0 is considered to be no pain, 1 to 3 is mild pain, 4 to 6 is moderate pain, 7 to 9 is intense pain and 10 is unbearable pain. For the descriptors, the 3 dimensions of the painful experience are considered. The scale was developed by Souza et al. (2010).
EUROHISQOL - 8. Is a quality of life assessment instrument derived from the WHOQOL-Bref. It consists of 8 items. Each of the domains (physical, psychological, social relationships and environment) is represented by two items. It consists of a global index, calculated from the sum of the eight items. A higher value corresponds to a better quality of life (UFRGS, 2018).
SOC Inventory (Selection, Optimization, Compensation), explains the concept of successful aging, developed by Baltes et al. (1999). In its original version it contains 48 items, however in this study the reduced version will be used, which was described by Freund and Baltes (2002) as more favorable. This version consists of 12 items that assess the use of SOC strategies by the elderly. Each item consists of two statements, one describing behavior reflecting the SOC and the other offering a reasonable but non-SOC-related option. The participant must decide which of the two alternatives characterizes their behavior.
Body Weight Status. Body mass was measured with a scale, which measures the subject's body weight (kg). For this assessment, the elderly person must stand, with their arms at their sides, without shoes and with as little clothing as possible. To measure height, a stadiometer will be used. The elderly person must be without shoes, with their feet together and with the posterior surfaces of the heels, buttocks and occipital region in contact with the measuring scale. The head must be aligned forming a line parallel to the ground. The elderly person evaluated must perform a maximum inspiration and a respiratory block. To calculate BMI, we used the calculation of the ratio between weight (kg) and height (m), using the formula: BMI = weight/height2. As determined by the Ministry of Health (Brasil, 2018), the cutoff points for the body weight status classification used were: < 22 kg/m2 = Low weight; ≥ 22 and ≤ 27 kg/m² = Adequate weight; > 27 kg/m² = Overweight.
International Physical Activity Questionnaire (IPAQ) was used to evaluate the practice of physical activities. It was used, in its long version, in the version adapted for the elderly. The IPAQ has short and long versions, which obtain answers about the four domains into which physical activity is divided for better understanding (leisure, commuting, work and domestic), but only the long version allows the analysis of each domain separately. The section refers to the physical activities that the elderly person did in the last week solely for recreation, sport, exercise or leisure. According to the objective of the study, it was decided to analyze only this domain, taking into account that the study sample is made up of elderly people who attend water aerobics classes at least once a week. In the adapted IPAQ, the questions referring to “the days” and “the time” of the different domains of physical activity were grouped together in the same question (which days and what time in a normal week and for 10 continuous minutes). The classification of the level of physical activity by IPAQ was carried out in accordance with the recommendation of the IPAQ coordinating center in Brazil - CELAFISCS (Benedetti et al., 2004; Benedetti et al., 2007; Mazo & Benedetti, 2010; Santos, 2013).
Results
The data analysis demonstrated, as shown in Table 1, how the groups are organized in relation to the presence and absence of musculoskeletal and osteoarticular disorders with the presence and absence of chronic pain. The Chi Square test results show is a significant difference between the groups (p=0.03), as we can see below. Thus, the greater the presence of musculoskeletal and osteoarticular diseases, the greater the presence of chronic pain, which can be identified in 81.8% of this group of elderly people.
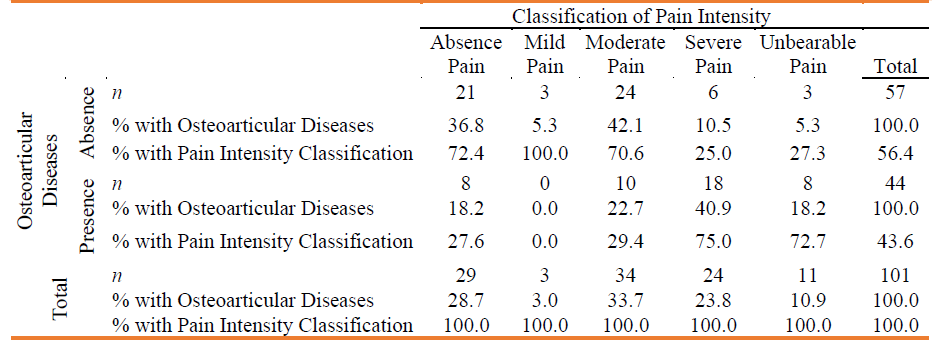
Table 2 shows that elderly people in the group with no musculoskeletal and osteoarticular disorders mostly have moderate pain, or do not have chronic pain, while elderly people with musculoskeletal and osteoarticular disorders are more concentrated in severe pain.
Table 1 Descriptive analysis of the relation between musculoskeletal and osteoarticular disorders and chronic pain (n=101)
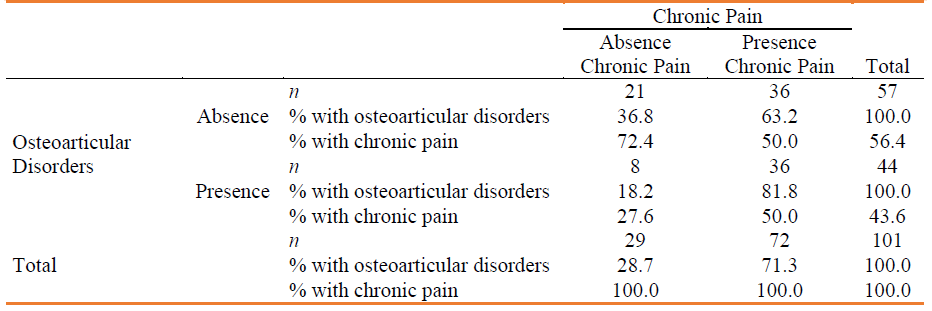
Table 2 Descriptive analysis of the relation between osteoarticular diseases and pain intensity (n = 101)
In the bivariate correlations, performed by using the Spearman test, separating the sample of elderly people who have no musculoskeletal and osteoarticular disorders and no chronic pain (n=21), the level of physical activity assessed by the IPAQ test demonstrated a moderate and direct relation with the successful aging strategy of elective selection, based on defined choices with greater autonomy (rho=0.541; p=0.014). The loss-based selection strategy presented a moderate and direct association (rho=0.571; p=0.009) with the optimization strategies and also with the compensation strategy (rho=0.624; p=0.003) that establishes a more appropriate form of aging and overcoming the inherent difficulties of the development process.
Stratifying the sample into groups of elderly people who have no musculoskeletal and osteoarticular disorders and the presence of chronic pain, we identified bivariate correlations, analyzed using the Spearman test. The Body Mass Index showed an indirect relation with the solicitude strategy (rho=-0.386; p=0.020), that is, the greater the overweight the less the strategy is used. The time of regular participation in the water aerobics activities of the project also has an indirect relationship with the loss-based selection strategy (rho=-0.439; p=0.007) and with solicitude (rho=-0.360; p=0.031) that contemplates the need for care and attention, due to the presence of chronic pain. Among the attitudes that affect behavior based on the complaint of pain, the use of medication has a direct relationship with emotion (rho=0.356; p=0.033) and with physical damage (rho=0.447; p=0.006). There was no correlation between the group of elderly people with the presence of musculoskeletal and osteoarticular disorders and absence of chronic pain, as it was a small sample, composed of only 8 individuals.
Table 3 shows the bivariate correlations stratifying the sample into groups of elderly people who have musculoskeletal and osteoarticular disorders and the presence of chronic pain. The physical activity level has a direct relation with the quality of life, showing that the practice of physical activity impacts on improving the quality of life of the elderly. The successful aging strategy based on compensation is directly related to the attitudes of emotion and solicitude, as well as the selection strategy based on losses. Therefore, it is clear that the presence of musculoskeletal and osteoarticular disorders and the presence of chronic pain leads to more fragile behavior and that requires care, attention and concern, revealing its implications for the successful aging process. Likewise, it affects the losses-based selection, resulting from the aging process.
The optimization strategy is indirectly related to solicitude, which composes attitudes towards the presence of chronic pain. The time of participation in the project also has an indirect relationship with the elective selection strategy, that is, the longer the time of participation of the elderly in the water aerobics project, the less the repercussion of losses in the elderly’s functionality.
In the group with musculoskeletal and osteoarticular disorders and chronic pain (n=36), linear regression analysis was performed using the stepwise method, with a significance level ≤ 0.05 and quality of life as the dependent variable.
Table 3 Correlation analysis in the group of elderly people with musculoskeletal and osteoarticular disorders associated with chronic pain
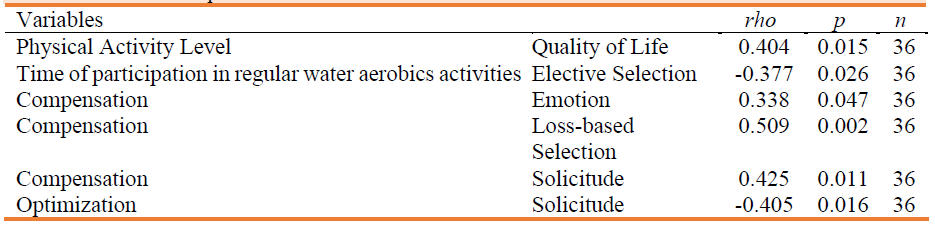
Table 4 Multiple Linear Regression of the quality of life variable in elderly people with musculoskeletal and osteoarticular disorders and chronic pain

In the analysis presented in table 4, the relation (signal and intensity) between the quality of life variable (dependent, explained) and the physical activity level variable (independent, explanatory) was verified. In this model, the R-squared (R 2 = 0.153) obtained indicates that the variations in quality of life can be explained by variations in the physical activity level of elderly people who have musculoskeletal and osteoarticular disorders and with the presence of chronic pain. In this group, it is clear that the promotion of the level of physical activity, combating physical inactivity, is associated with an increase in the perception of quality of life.
In the group with absence of musculoskeletal and osteoarticular disorders and presence of chronic pain (n=36), linear regression analysis was performed by using the stepwise method, with a ≤ 0.05 significance level and a dependent variable to strategies for successful aging (Selection, Optimization and Compensation).
Table 5 Multiple Linear Regression of successful aging strategies (SOC) in elderly people with diseases

In the analysis presented in Table 5, a direct relation between successful aging strategy (dependent, explained) and the body mass index variable was verified, whereas an indirect relation with the time of participation in the water aerobics project was present. In this model, the R-squared (R 2 = 0.250) indicated that the variations in successful aging strategies can be explained by variations in BMI and time of participation in the project. In this group, the promotion of successful aging is associated with the practice of water aerobics and the control of body weight.
Discussion
The outcomes of this study are due to the analysis of the relation between musculoskeletal and osteoarticular disorders with chronic pain in elderly people who practice water aerobics. In regard to the presence of chronic pain, the results obtained in this study are in line with epidemiological studies referred to in the study by Gibson and Lussier (2012), ratifying the presence of pain in the late phase of life and its continuity in approximately the same prevalence until the most advanced age. Therefore, chronic pain present in the daily life of elderly people is a considerable risk factor for the development of disabilities. Considering the presence of osteoarticular and musculoskeletal diseases in relation to the intensity of chronic pain, the results of this study showed that the predominant intensity is severe, also revealed in the study by Severina et al. (2018). In a study with 451 elderly municipal employees in Londrina, most pain complaints had their intensity ranging from moderate to severe (Dellaroza & Pimenta, 2012).
In line with the results found in this study, the study by Kostadinovic et al. (2019) reveals long-term health problems significantly associated with pain, particularly at moderate and severe levels, as elderly people with long-term health problems had almost twice the risk of a moderate degree of pain and more than double the risk of a severe degree of pain.
In regard to the analysis of the group of elderly people with no musculoskeletal and osteoarticular disorders and no chronic pain, the results of this study showed a relation between the level of physical activity and greater autonomy for the elderly in choosing successful aging strategies. The loss-based selection strategy occurs in significant association with optimization strategies, which indicates the maintenance of the skills that are still preserved and the compensation that is intended to make up for the compromised skills. In this context, it is important to refer to the aspects that integrate the concept of successful aging, defended by Simões (2006), constituted of low risk of diseases or disabilities related to the disease, high physical and mental functioning and active engagement in life. Therefore, the author highlights people’s attitude towards their own lives, in order to prevent disease and promote health.
With the decline in functional capacities, the elderly use strategies to maintain personal performance in tasks that were already performed. In order to compensate for the normative losses of the aging process and improve the methods and the way they are performed (Lima et al., 2008). In the context of successful aging, the outcomes of this study indicate a relationship between the compensation strategy, based on new dynamics due to the deleterious effects of the aging process, with loss-based selection, with repercussions on individual and social activities. The strategy also shows a relation with solicitude and emotion, both attitudes characterized by the complaint of pain. There is also a significant relation between the optimization strategy and solicitude, indicating the activation of means that reduce the need for care and attention in the presence of chronic pain. Another relevant aspect reveals a significant association between successful aging strategies with the practice of water aerobics and body weight control in the group of elderly people who manifest osteoarticular and musculoskeletal disorders and chronic pain.
Given this scenario, the benefits of performing physical activities are equally evident for the adequate intellectual, physical, affective and social functioning. There is sufficient data to state that a strong and positive relation between physical activity and successful aging is present, ensuring that people who remain active continue physical functioning. In addition, the possibility of delaying normal decline related to the complexity of a process that goes beyond the biological cycle is associated, reaching undeniable psychological and socio-cultural benefits (Gomes & Britto, 2009).
Considering the mechanisms that involve studies on successful development, aging that occurs concurrently with the practice of physical activities can be considered as a process to optimize health, participation and safety opportunities. This process promotes the improvement of the quality of life of the elderly and, currently, it is one of the main references in policies aimed at elderly people (Marinho et al., 2016).
In this context, this study found a significant correlation between the level of physical activity and quality of life, demonstrating that the presence of chronic pain and osteoarticular and musculoskeletal disorders does not hinder the involvement in physical activities. Within this perspective, the study by Oliveira et al. (2014) found the effectiveness of an exercise program to control pain processes, with a significant decrease in the pain threshold.
Similar results were found in the study by Silva et al. (2016), in which the majority of elderly people evaluated their own quality of life as positive and revealed that physical activity contributed a lot to make this happen, highlighting the physical and emotional aspects. In this study, the authors refer to the friendships developed during the activities. In the pain-related domain, the study revealed a significant decline in quality of life, noting that pain is a factor that limits functions and impairs the daily activities of the elderly.
The results of the studies by Lini et al. (2016) and Krug et al. (2013) showed the presence of chronic pain with a predominant location in the lower and upper limbs, lumbar and cervical spine, as obstacles to the practice of physical activities. The study by Lini et al. (2016) also showed that the complaint of chronic pain has a direct and negative relationship with self-rated health, and compromises functionality for carrying out basic activities of daily living.
The results found in the study by Ferretti et al. (2018) showed that the presence of chronic pain, a greater number of diseases and high pain intensity negatively influenced the quality of life of the elderly studied, thus evidencing implications for quality of life, due to complaints of chronic pain. Regarding the practice of physical activity, the same study observed a weak and negative correlation between the volume of physical activity practiced with the intensity of pain and the number of chronic diseases in elderly women, and the level of physical activity decreased with increasing intensity of pain and the number of chronic diseases. The study also revealed that elderly women with chronic pain have a significantly lower frequency of practice than those who do not have chronic pain.
Physical, psychological and social disabilities are the main repercussions that affect the quality of life of elderly people with chronic pain, and its identification is important. In this context, the study by Cunha and Mayrink (2011) showed the presence of moderate pain assessed by the one-dimensional scale, with negative influences on the quality of life of the elderly. The results showed a weak correlation in the physical and psychological domains and an absence of correlation in the social relations, environment and pain intensity domains. Arguing the occurrence to the fact that the evaluation instrument is one-dimensional and evaluating only the intensity of pain, which was moderate.
In view of the different complications of the presence of osteoarticular and musculoskeletal disorders and chronic pain in the health and quality of life of the elderly, it is possible to verify that these events are not impediments to the practice of physical activities. Likewise, it is considered important to refer to the type of activity, taking into account that the elderly people in this study practice water aerobics, which is a physical activity consisting of specific exercises, which provides a lower risk of joint pain due to the decrease in impact strength caused by weight, which is minimized in the water. The movements performed in the aquatic environment provide greater amplitude and allow for a smoother performance and less risk of pain (Baun, 2010).
In conclusion, based on these results, the presence of osteoarticular and musculoskeletal diseases, as well as complaints of chronic pain, are not impediments to the practice of regular physical activity. It is perceived that the choice of water aerobics activity is linked to osteoarticular and musculoskeletal disorders, with repercussions on improving functionality and quality of life within the scope of successful aging. In this sense, it is worth highlighting the relevance of this activity as an opportunity to prevent and promote the health of the elderly, taking into account the uniqueness and complexity of the biological, psychological and social aspects that make up the active aging process. Likewise, it seems relevant to make reference to municipal actions, highlighting the implications of this intervention model on the health of the elderly population.
Contribuição dos autores
Anna Barcelos: Concetualização; Análise formal; Investigação; Metodologia; Redação do rascunho original; Redação - revisão e edição.
Caroline Fagundes: Investigação; Redação - revisão e edição.
Andrea Dani: Investigação; Redação - revisão e edição.
Martina Scur: Redação - revisão e edição.
Daiane Berlese: Concetualização; Metodologia; Redação - revisão e edição.
Geraldine Santos: Concetualização; Curadoria dos dados; Análise formal; Aquisição de financiamento; Metodologia; Administração do projeto; Supervisão; Redação do rascunho original; Redação - revisão e edição.

