











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
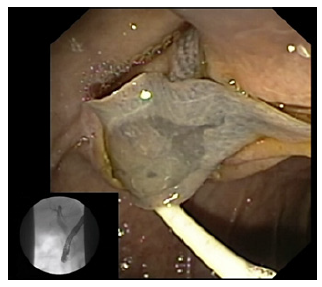
PermalinkThe authors report 3 cases of different patients with biliary parasitosis, diagnosed, and treated by endoscopic retrograde cholangiopancreatography (ERCP) (online suppl. video). All patients denied relevant risk factors for parasitosis, namely environmental, hygiene, or dietary factors. The first 2 cases illustrate biliary colonization by Fasciola hepatica. One of these patients presented with obstructive jaundice and the other with recurrent pancreatitis (two previous acute pancreatitis with mild dilation of extrahepatic bile ducts with biliary sludge in the common bile duct, described on emergency ultrasound). In the first case, abdominal ultrasound was suggestive of biliary parasites. In both patients, cholangiography performed during ERCP revealed multiple small filling defects with elliptic and sigmoidal shapes in the main bile duct with common bile duct dilation. After clearance of the bile ducts using an extraction balloon, the diagnosis was confirmed to be biliary parasitosis due to Fasciola hepatica. In the second case, the parasite was retrieved alive (shown in Fig. 1). Each patient received complementary treatment with triclabendazole the day after the endoscopic procedure at a dose of 10 mg/kg orally twice daily for 2 days.
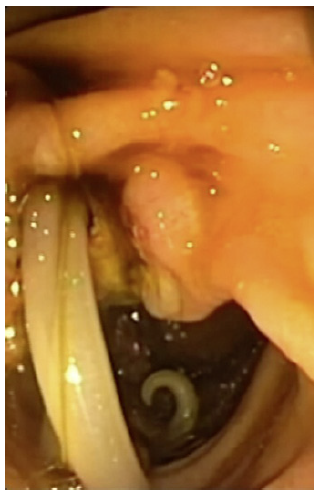
The third case corresponds to a patient that presented with acute cholangitis. During ERCP, cholangiography revealed many elongated irregular filling defects and dilation of the common bile duct without intrahepatic duct dilation. After performing sphincterotomy, the bile duct was cleared using a Dormia basket and a balloon extractor, allowing the removal of Ascaris lumbricoides already without motility (shown in Fig. 2). Endoscopic treatment was also supplemented with albendazole 400 mg orally as a single dose the day after the procedure. All patients had significant clinical improvement shortly after ERCP and have been discharged asymptomatic after 3 days.
In Portugal, as in other developed countries, biliary parasitosis are rare diseases. However, the incidence of these infestations appears to be increasing in line with the increase in tourism and immigration. Diagnosis is usually supported by ultrasound, computed tomography, magnetic resonance imaging (MRI), or endoscopic ultrasound [1]. Although ERCP is mainly used for therapeutic aspects, in rare cases ERCP is the key to the diagnosis [2]. We intend to illustrate the typical findings of parasitosis in cholangiography and duodenoscopy and demonstrate the usefulness of ERCP in the diagnosis and treatment of biliary obstructions due to biliary parasitosis.

