










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPortuguese Journal of Nephrology & Hypertension
versão impressa ISSN 0872-0169
Port J Nephrol Hypert vol.32 no.3 Lisboa set. 2018
ORIGINAL ARTICLE
Peritoneal dialysis catheter placement with percutaneous technique with fluoroscopic guidance – our centers experience
Joana R. Silva, Ricardo A. Macau, Joana M. Martins, Jorge Silva, Fernando T. Costa, Aura Ramos
Nephrology Department, Hospital Garcia de Orta, Portugal
ABSTRACT
Introduction: Studies have shown no clear superiority between surgical and percutaneous methods for peritoneal dialysis (PD) catheter insertion, so the preferred method usually depends on each centers experience. In our center we perform both percutaneous technique with fluoroscopic guidance (PTFG) and laparoscopic technique (LT).
Objective: Our main goal is to present our experience with PTFG and our results. We also aim to compare PTFG with LT in terms of complications associated with catheter placement and 1-year catheter survival.
Methods: We performed a retrospective study that included the 17 incident patients submitted to first PD catheter placement using PTFG from 28th October 2014 to 15th March 2018 and the last equivalent number of patients that were submitted to first PD catheter placement using LT, until 15th March 2018.
Results: We observed no statistically significant differences between groups with respect to 1-year catheter survival and complications related to PD catheter insertion, apart from dialysate leakage, which was higher in the LT group. There were complications to take into account in the PTFG group.
Conclusion: PTFG performed by nephrologists seems to be an effective technique for PD catheter placement, although no substitution for surgical techniques when clinically indicated, and results can be improved with increased experience with this technique.
Keywords: Peritoneal dialysis, peritoneal dialysis catheter, percutaneous, fluoroscopy, laparoscopy.
INTRODUCTION
Peritoneal dialysis (PD) is an effective method of renal replacement therapy, and appears to have some advantages over hemodialysis in terms of improved survival in the first years after initiation of dialysis, costs, preservation of residual renal function and quality of life1,2. The success of this modality is dependent on timely and adequate peritoneal access2.
There are different options for catheter insertion in the peritoneal cavity, which include surgical procedures (open, laparoscopic and peritoneoscopic) and percutaneous procedures (Seldinger and modified Seldinger, with or without radiologic guidance)1-3.
Meta-analyses have demonstrated no advantage of laparoscopic over open surgical placement and smallscale studies have suggested that the percutaneous method is effective and may have a lower rate of complications than surgical techniques2. A recent metaanalysis that attempted to clarify the comparison of the outcomes of percutaneous and surgical techniques (such as 1-year catheter survival, infectious complications and mechanic complications) concluded that the incidence of overall infections and mechanical complications was more frequent in the surgery group than the percutaneous group, but there was no difference in the 1-year catheter survival rate1. The percutaneous techniques seemed to be an effective and safe alternative to surgical techniques and should be considered in selected patients (such as those with no prior abdominal surgeries and body mass index < 28 kg/m2)1. A prospective randomized trial by Voss et al that included 113 patients and compared fluoroscopically guided versus surgical insertion of first catheter for PD concluded that radiological insertion of first PD catheters using fluoroscopy was a clinically non-inferior and cost-effective alternative to surgical laparoscopic insertion4.
According to the 2010 International Society for Peritoneal Dialysis (ISPD) guidelines for peritoneal access, the preferred PD catheter implantation technique should depend on each centers experience5.
Currently in our center we use both percutaneous technique with fluoroscopic control (PTFG) and laparoscopic technique (LT). Our center has used percutaneous and surgical PD catheter placement techniques.
The risks of general anesthesia in very comorbid patients and the long waiting times for availability of operating rooms led to an interest in gaining experience with percutaneous techniques, performed by nephrologists.
Blind percutaneous Seldinger technique was used until October 2014, when fluoroscopic guidance was added to better visualize catheter placement and avoid complications, namely catheter misplacement. We still tend to prefer LT in patients with past history of multiple intra-abdominal surgeries, organomegalies (such as polycystic kidneys) and abdominal hernias; however, each case is evaluated individually.
Our main goal is to present our experience with PTFG and our results. We also aim to compare PTFG with LT in terms of complications associated with catheter placement and 1-year catheter survival.
MATERIALS AND METHODS
We performed a retrospective study in which we revised epidemiologic and clinical information of patients from the PD program in our center.
The following patients were included: 1) Incident patients that were submitted to first PD catheter placement using PTFG from 28th October 2014 to 15th March 2018; 2) The last equivalent number of patients that were submitted to first PD catheter placement using LT, until 15th March 2018.
We collected the following data for each patient: gender, age at time of PD catheter placement, etiology of kidney disease, history of diabetes (type 1 or 2), previous abdominal surgeries, previous renal replacement therapies, reasons for entering PD program, time of PD catheter placement, time of PD start, time to withdrawal from PD program (if applicable, complications related to catheter placement and catheter patency at 1 year. We were not able to ascertain the patients body mass index at the time of catheter placement.
The complications related to catheter placement were designated in accordance with the audit of PD catheter insertion from the guidelines of the International Society for Peritoneal Dialysis, 2010: bowel perforation, significant hemorrhage, dialysate fluid leak, exit-site infection within 2 weeks after catheter insertion, peritonitis within 2 weeks after catheter insertion, catheter dysfunction at the time of first use that requires catheter manipulation or replacement or results in technique5.
All catheters placed were double cuffed, swan neck, coiled. PD catheter insertion with PTFG. This technique is performed by a fixed team of nephrologists in an angiographic procedures suite, with administration of 5 mg oral diazepam and local anesthesia. The patients are admitted on the day prior to the procedure, when bowel preparation is performed. Prophylactic vancomycin (1g intravenous) is administered half an hour before the procedure. The procedure includes the following steps: 1) the patient is positioned in supine; 2) trichotomy and sterilization are performed; 3) the catheter entrance (punction site) and exit sites are defined using the catheter about to be placed and fluoroscopic imaging. The catheter entrance site (punction site) is 2 to 4 cm lateral to the medial abdominal line, in the middle of the rectus muscle, and the external cuff must be 2 to 4 cm from the exit site; 4) the exit site is marked with a punch used for dermatological biopsies; 5) local anesthesia of the punction site is made with 2% lidocaine; 6) the needle is inserted until it reaches the peritoneal cavity. If there is doubt about the position of the needle, contrast (3-5 cc) is injected through the needle and the intestinal contours are visualized with fluoroscopy. The needle is fixed in its position and 1000 cc of normal saline at 36ºC are injected through the needle; 7) the guiding wire is inserted through the needle into the peritoneal cavity under fluoroscopic control; 8) the paired dilator/sheath is inserted; 9) the dilator is removed and the catheter is introduced through the sheath, under fluoroscopic control. If there is any doubt about positioning of the catheter, contrast can be injected through the catheter to confirm its correct position; 10) the catheter is tunneled; 11) the injected saline is drained, the catheter is tested and finally the internal catheter entrance site is stitched. PD catheter insertion with LT. This technique is performed by a fixed team of general surgeons according to standard LT procedures and the laparoscope brand.
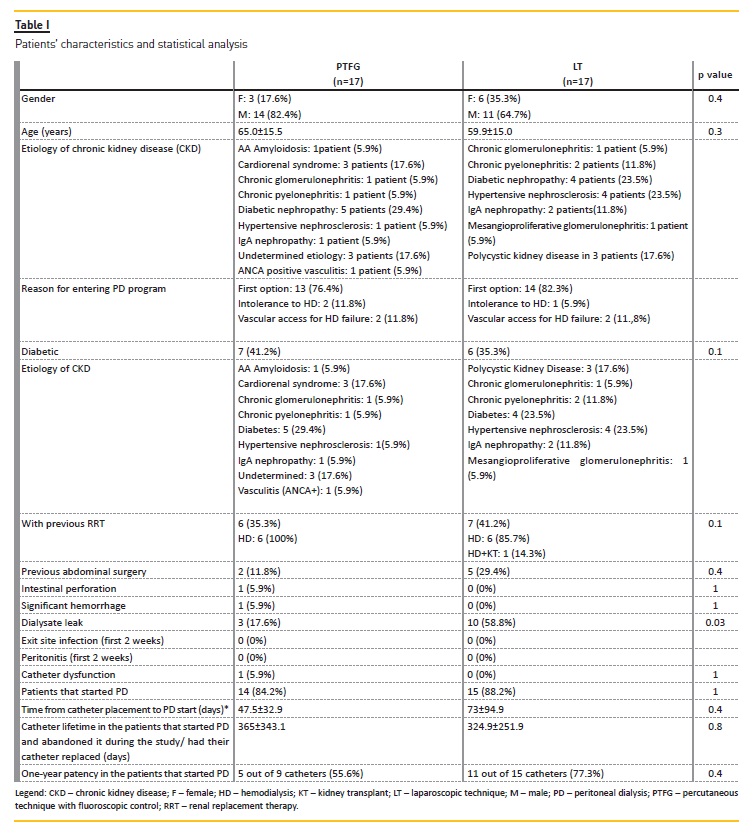
Rectus sheath tunneling is performed, as well as omentopexy and adhesiolysis, if necessary. Statistical analysis was performed using SPSS statistics 23®. To compare the techniques, we used the chisquare test or Fishers exact test for categorical variable (gender, diabetes, previous renal replacement technique, previous abdominal surgery, complications of the technique and 1-year catheter patency) and the t test for continuous variables (age, time from catheter placement to PD start and catheter lifetime). p value level of significance was fixed at < 0.05 (Table I).
RESULTS
In the period between 28th October 2014 and 15th March 2018, 17 first PD catheters were inserted with PTFG. We selected the last 17 first PD catheters inserted with LT. Out of the 17 catheters placed with PTFG, 7 were placed in 2017 (41.2%) and 2 in 2018 (17.6%) and out of the 17 catheters placed with LT, only 2 were placed in 2017 (17.6%) and none in 2018, by the time of the end of our study.
The patients characteristics and comparison between techniques are summarized in Table I.
Average age at the time of catheter placement was 65±15.5 years in the PTFG group and 59.9±15,0 years in the LT group (p=0.3).
In the PTFG group, 14 patients (82.4%) were male and 3 female (17.6%), and in the LT group, 11 patients (64.7%) were male and 6 female (35.3%) (p=0.4).
The etiologies of chronic kidney disease (CKD) in the PTFG and LT groups are presented in Table I.
Seven patients (41.2%) in the PTFG group and 6 patients (35.3%) in the LT group had diabetes (p=0.1). Two patients (11.8%) in the PTFG group and 5 patients (29.4%) in the LT group had had previous abdominal surgery (p=0.1). In the PTFG group both procedures were appendectomies and in the LT group the procedures were augmentation enterocistoplasty (1 patient [20%]), appendectomy (1 patient [20%]), nephrectomy (1 patient [20%]), hysterectomy (1 patient [20%]) and inguinal herniorrhaphy (1 patient [20%]).
Thirteen patients (76.4%) in the PTFG group and 14 patients (82,3%) in the LT group entered the PD program due to personal preference over HD. The remaining patients entered the PD program either due to intolerance to hemodialysis (HD) or failure of vascular access for HD (Table I).
Six patients (35.3%) in the PTFG group and 7 patients (41.2%) in the LT group had had previous renal replacement therapy. 6 patients in the PTFG group and 7 patients in the LT group had been submitted to HD (some of them temporarily, in the transition period to PD) and 1 patient in the LT group had also been submitted to kidney transplantation, and had a failing graft at the time.
In the PTFG group, by the end of the study, fourteen patients (82.4%) started PD. One patient (5.8%) was still in training and 2 patients (17.6%) did not start PD due to complications: bowel perforation with fecal peritonitis (1 patient) and Pseudomonas aeruginosa peritonitis on the 16th day after catheter placement, with associated catheter malfunction (1 patient). Of the patients that started PD, average time from catheter placement to beginning of the technique was 47.5±32.9 days and, by the time of end of the study, out of the patients that had started PD, 7 patients (50%) were still in the PD program. Average at use lifetime of the catheter in the patients that left the PD program was 365 ± 328.5 days.
In the LT group, by the end of the study, fifteen patients (88.2%) started PD. Two patients (11.8%) didnt start PD because they chose to switch to HD. Of the patients that started PD, average time from catheter placement to beginning of the technique was 73 ± 109.5 days, and, by the time of the end of the study, out of the patients that had started PD, 7 patients (46.7%) were still in the PD program, while 8 patients (53.3%) abandoned the program. In one patient, the catheter was replaced after displacement and associated dysfunction and concomitant exit-site infection. This occurred 153 days after catheter placement. Average at use lifetime of the catheter in the patients that left the PD program plus the patient that had his catheter replaced was 324.9 ± 251.9 days.
We evaluated and compared the complications associated with PD catheter placement with PTFG and associated with LT (Table I):
Bowel perforation. One case (5.9%) of bowel perforation occurred in the PTFG group, and none occurred in the LT group (p=1). The only case of bowel perforation occurred in a patient that had a past history of appendectomy and was uncompliant with standing still during the procedure. The procedure was immediately interrupted and the surgical team was informed. The patient had to be submitted to surgery due to fecal peritonitis. He recovered well, but had to be switched to HD.
Significant hemorrhage. Two cases (11.8%) of significant hemorrhage occurred in the PTFG group, and none occurred in the LT group (p=0.4). In one of the patients, the procedure incurred no problems and no hemorrhage was detected; however 2 days after the procedure the patient developed hemodynamic instability as well as a drop in hemoglobin. Decision was made to bring the patient to the operating room, where hemorrhage from superficial epigastric vein was detected.
The patient started PD after 3 months; in another patient, a small hemorrhage was detected in the tunnel on the 3rd day after the procedure and was managed with a hemostatic stitch.
Dialysate leak. Three cases (17.6%) of leak occurred in the PTFG group, and 10 cases (58.8%) occurred in the LT group (p=0.03). Average time from catheter insertion to leak detection was 3.3±3.2 days in the PTFG group and 6.3±4.4 days in the LT group (p=0,3). All leaks were detected before starting PD, during catheter lavages, and all resolved with rest and did not preclude starting PD.
Exit-site infection within 2 weeks of catheter insertion. No cases were observed of exit-site infection within 2 weeks (14 days) of catheter insertion in either of the groups. It is worth mentioning; however, that one patient in the PTFG group was diagnosed with exitsite infection (Pseudomonas aeruginosa) 16 days after catheter insertion.
Peritonitis within 2 weeks of catheter insertion. No cases were observed of peritonitis within 2 weeks (14 days) of catheter insertion in either of the groups. It is worth mentioning however, that one patient in the PTFG group was diagnosed with peritonitis (methicillinresistant Staphylococcus aureus) 16 days after catheterinsertion. This was the same patient that had exit-site infection 16 days after catheter infection.
Functional catheter problem requiring manipulation or replacement or leading to technique failure. One case (6%) occurred in the PTFG group and 1 case (6%) occurred in the LT group. In the PTFG group one patients catheter became displaced and occluded 25 days after placement and was repositioned surgically. In the LT group one patients catheter became displaced and occluded 153 days after placement and, since the patient had exit-site infection, this catheter was removed and another catheter placed on the opposite site, at the same time, in the operating room.
We also evaluated catheter survival at 1 year. Out of the 14 patients in the PTFG group that started PD, 9 (64.3%) had had their catheters inserted at least 1 year before the end of the study. Five (55.,6%) of the patients had patent catheters at 1 year; the remaining patients abandoned the program. All the 15 patients that started PD in the LT group had had their catheters inserted at least one year before the end of the study. Eleven (73.3%) of the patients had patent catheters at 1 year; the remaining patients abandoned the program.
DISCUSSION
As previously stated, peritoneal dialysis (PD) has clinical advantages, and a timely and well-functioning inserted PD catheter is key for its success1,2.
Meta-analyses have shown that percutaneous placement of PD catheters is effective and safe1,2. Moreover, implementation of this technique by nephrologists has shown a capability to stimulate the growth of PD programs, as described by Asif et al7.
Towards the end of 2017, percutaneous procedures increased in our PD unit, due to nephrologists increasing experience with PTFG and the need for timely insertion of catheters coupled with long waiting times for operating rooms for surgical procedures.
In our study, the LT and PTFG groups had similar demographics in terms of gender, age, diagnosis of diabetes, previous renal replacement therapies and previous abdominal surgery.
Both the cause of chronic kidney disease and the reasoning behind choosing PD modality can have an impact on our choice of the technique. For instance, patients with cardiovascular instability and intolerance to hemodialysis might benefit from avoidance of general anesthesia, and patients with polycystic kidney disease might benefit from a surgical procedure.
In literature, reported exclusion criteria for the percutaneous technique include obesity, hernias, previous peritonitis, previous abdominal surgery and polycystic kidney disease. On the other hand, patients with unsuitable conditions and high risk surgical candidates are usually excluded from surgical techniques2.
Hauch et al evaluated the role of laparoscopic techniques in patients with difficult abdomen. In their study, major abdominal surgery was defined as a laparoscopic or open intraperitoneal procedure that would typically last > 30 minutes6. LT was attempted in a cohort of 120 patients. Whenever needed, adhesiolysis, omentopexy and hernia repair were performed. Of the 120 patients, 47.4% had had previous major abdominal surgery. The complication rates between patients with or without previous abdominal surgery did not differ.
Notably, however, more adjunctive procedures such as adhesiolysis and hernia repair were performed in patients with previous abdominal surgery6.
In our unit, patients with previous complex abdominal surgery, polycystic kidney disease and with hernias are usually triaged to LT. However, we evaluate each case individually; hence, two patients with previous uncomplicated appendectomies were not excluded from PTFG. Perhaps because the sample was too small, past history of abdominal surgery did not statistically differ between PTFG and LT groups, respectively: 2 patients (11.8%) versus 5 patients (29.4%, p=0.4). In the PTFG group, we reported bowel perforation in 1 patient with previous appendectomy (5.9%).
De Boo et al performed a review of the literature on percutaneous insertion of peritoneal dialysis catheters using X-ray guidance with or without ultrasound guidance3.
Some of the studies included in the analysis excluded from the percutaneous technique patients with previous abdominal surgery3,4,7,8. Zaman et al used fluoroscopic guidance and excluded patients with multiple previous abdominal surgeries or previous PD catheters.
They reported a success rate of 94% and no bowel perforations3,7. Maya et al used fluoroscopic and ultrasound (US) guidance and included patients with some abdominal surgeries such as cholecystectomy, cesarean section and hysterectomy. They reported a success rate of 94% and an incidence of 3% of bowel perforations3,8.
Vaux et al used fluoroscopic and US guidance and excluded patients with previous abdominal surgery. They reported a success rate of 94% and no bowel perforations.
Voss et al used fluoroscopic guidance and excluded patients with previous abdominal surgery or a history consistent with adhesions. They reported a success rate of 98% and no bowel perforations3,4. De Boo et al also reported their own experience with percutaneous modified Seldinger technique with fluoroscopic and US guidance: 33 patients of their cohort (87%) had had previous abdominal surgery (of whom, 88% with opening of the peritoneal cavity). There was a 100% success rate in their cohort and no bowel perforations3.
Based on our own results and the evidence in the literature, we believe patients with past abdominal surgery, especially if involving peritoneal manipulation, should be regarded with caution and preferably managed with LT.
We observed one case of significant hemorrhage, in the PTFG group (5.9%). Although in theory the addition of US guidance could minimize the risk of bowel and bladder perforation and injury to the abdominal vessels, in the review by De Boo et al it was verified that hollow organ puncture was observed in 0.9% of X-ray guided insertions versus 1.0% of combined X-ray and US-guided insertions, and no significant hemorrhage was reported.
In their own cohort, De Boo et al used both US and fluoroscopy guidance and, as previously mentioned, no patient suffered from bowel puncture; however, 3 patients (3%) suffered from exit-site bleeding and in one of those patients, bleeding resulted in removal of the catheter3. Based on our results and the literature, we do not consider that there is enough evidence to support adding US guidance to our procedure.
Percutaneous procedures with radiological control have been performed under conscious sedation with intravenous fentanyl and midazolam7-11, intravenous morphine12 or intramuscular pethidine13, in addition to local anesthesia. Vaux et al found that conscious sedation and narcotic analgesia was rarely needed (used in only 2.3% of their cohort)15. We use diazepam and local anesthesia during PTFG. If possible, we may ask for the patients collaboration in some parts of the procedure, in voluntarily contracting the abdominal muscles when asked to do so (for instance, during needle and dilator/sheath insertion). The patients must be well aware that they will be conscious throughout the procedure, and some anxious patients prefer LT for this reason.
The only statistical difference observed between groups with respect to catheter insertion-related complications, was dialysate leak, where PTFG was superior (17.6 versus 58,8%, p=0.03).
A dialysate leak occurs as a consequence of the loss of the peritoneal membrane integrity. In terms of timing, leaks can occur early (within 30 days) or late, after catheter insertion. Early leaks can be associated with the insertion technique and the timing of, and volumes used in, PD initiation, while late leaks are usually associated with the existence of weaknesses in the abdominal wall16.
An association has been found between early leaks and immediate PD initiation16. Tzamaloukas et al studied early and late leaks in patients on continuous ambulatory PD, and found that all early leaks developed in patients who started PD immediately after insertion of the PD catheter (90% within 10 days and more than half within 24h)16.
In our study, time from catheter placement to PD start did not differ between groups. We noticed a large inter-patient variation that might be related to factors other than the insertion technique itself, such as patient ability to learn the technique and urgency to start PD due to loss of kidney function. The average time in both groups was superior to two weeks, which is in accordance with the Peritoneal Access Guidelines of the ISPD that suggest that PD start should be withheld until after 2 weeks of PD catheter insertion5.
Early leakage most often manifests as an exit-site (or pericatheter) leak, which is often not apparent until the patient resumes normal activity and starts PD exchanges, but can also appear during initial peritoneal lavage16. All the leaks observed in our patients were early exit-site leaks, detected during small instillation of dialysate volumes (peritoneal lavages), before actual PD start. Though not consensual amongst PD units, we find the instillation of small volumes of dialysate useful to check for healing of the exit-site and tunnel around the catheter, before actually starting PD. If a leakage is detected, as happened in some of our patients, we stop instillation of volumes temporarily and do not start volume exchanges unless clinically urgent. All cases of leakage were successfully managed with pause in instillation of fluid, and none precluded PD start. The reason why more leaks were observed in the LT group might be related to technical differences between procedures; however our sample is too small to draw conclusions.
In the literature, leaks have been associated with a median surgical approach; however this has not been consistent in all cohorts16. Moreover, a retrospective analysis of 313 PD catheter insertions comparing percutaneous Seldinger with open surgical techniques showed higher rates of exit-site leaks in the percutaneous group (20.5% versus 6.8%, p=0.002)2.
In the literature, the incidence of dialysate leakage is > 5%, which according to Leblanc et al probably underestimates the number of early leaks associated with a more favourable outcome and that may be overlooked in a retrospective review16. In the review of percutaneous techniques with radiological control (De Boo et al), the incidence of exit-site leakage varied between 0 and 10%3. In our study, both techniques presented higher rates of dialysate leak than those seen in literature. This could be related to peritoneal lavages, but could also be due to overlooking of dialysate leaks with small clinical impact in retrospective studies.
A recent meta-analysis suggested that peritonitis rates may be higher with surgical techniques, but stronger studies are needed to confirm this2. Early peritonitis rates in percutaneous techniques with radiologic guidance vary from 0% to 16%3. In our study none of the groups had infectious complications within 2 weeks of catheter insertion, which is the time interval in which an infection might be associated with the technique of PD catheter insertion, according to the 2010 ISPD guidelines5. The fact that studies might have used a different time interval could have affected the results.
Only one patient in the PTFG group (5.9%) experienced catheter dysfunction with the need for surgical correction. In our unit, whenever the catheters are dysfunctional, they are repositioned or replaced surgically.
Catheter dysfunction rates in percutaneous techniques with radiologic guidance vary from 0% to 20%9.
One-year catheter survival was similar between PTFG and LT (respectively 55.6 versus 73.3 %, p=0.4).
Recent meta-analysis found no differences in 1-year survival in percutaneous versus surgical PD catheter placement1,2.
Though our complication rates with the PTFG technique were, apart from dialysate leak and significant hemorrhage, similar to the ones verified in literature for percutaneous techniques with radiological control, we performed suboptimally with respect to the audit standards for catheter related complications of the ISPD. We did not accomplish < 1% rates of bowel perforation and < 1% rates of significant hemorrhage, though we accomplished < 5% rates of exit-site infection and peritonitis and < 20% rates of catheter dysfunction.
The verified complications could be related to the selection of patients (namely patients with previous abdominal surgery), their own comorbidities, the procedure itself or the learning curve of the nephrologists that perform this technique.
Since the addition of fluoroscopy is recent, our sample is small, so we were unable to draw strong conclusions. Based on our results and the literature, PTFG seems to be an effective technique for PD catheter placement and an alternative to LT in certain clinical circumstances, though not substitutive.
The fact that the nephrology team dedicated to PTFG is a fixed one will allow for a progressive increase in experience. We expect to continue performing PTFG and improve our results.
CONCLUSION
In our PD unit, both percutaneous and surgical techniques have been used for PD catheter insertion. Nephrologists use a percutaneous Seldinger technique that was previously blind but is currently performed under fluoroscopic guidance. PTFG seems to be an effective alternative to LT, but not substitutive.
As a percutaneous technique, PTFG has the advantages of less time on waiting list for operating rooms and the avoidance of general anesthesia. The addition of fluoroscopic control allows for a better visualization of catheter positioning.
Surgical techniques such as LT allow PD catheter placement in the difficult abdomen and the performance of hernia repair, omentopexy and adhesiolysis if necessary.
Though our results were, for the most, similar to the ones verified in literature for percutaneous techniques with radiological control, we performed suboptimally with respect to the audit standards for catheter related complications of the ISPD and we hope to improve our results with increased experience.
References
1. Tullavardhana T, Akranurakkul P, Ungkitphaiboon W, Songtish D. Surgical versus percutaneous techniques for peritoneal dialysis catheter placement: a meta-analysis of the outcomes. Ann Med Surg (Lond). 2016; 10: 11-18 [ Links ]
2. Boujelbane L, Fu N, Chapla K, Melnick D, Redfield RR, Waheed S, Yevzlin AS, Shin JI, Astor BC, Chan MR. Percutaneous versus surgical insertion of PD catheters in dialysis patients: a meta-analysis. J Vasc Access. 2015; 16: 498-505 [ Links ]
3. De Boo DW, Mott N, Tregaskis P, Quach T, Menahem S, Walker RG, et al. Percutaneous insertion of peritoneal dialysis catheters using ultrasound and fluoroscopic guidance: a single centre experience and review of literature. J Med Imaging Radiat Oncol. 2015; 59(6): 662-667 [ Links ]
4. Voss D, et al. Radiological versus surgical implantation of first catheter for peritoneal dialysis: a randomized non-inferiority trial. Nephrol Dial Transplant. 2012; 27: 4196-4204 [ Links ]
5. Figueiredo A, Goh BL, Jenkins S, Johnson DW, Mactier R, Ramalakshmi S, et al. Clinical practice guidelines for peritoneal access. Perit Dial Int. 2010; 30: 424-429 [ Links ]
6. Hauch AT, Lundberg PW, Paramesh A. Laparoscopic techniques enable peritoneal dialysis in the difficult abdomen. JSLS. 2014; 18 (4): e2014.002334 [ Links ]
7. Zaman F, Pervez A, Atray NK, Murphy S, Work J, Abreo KD. Fluoroscopy-assisted placement of peritoneal dialysis catheters by nephrologists. Semin Dial. 2005; (3): 247-251 [ Links ]
8. Maya, ID. Ultrasound/fluoroscopy-assisted placement of peritoneal dialysis catheters. Semin Dial. 2007; 20(6): 611-615. [ Links ]
9. Savader SJ, Geschwind JF, Lund GB, Scheel PJ. Percutaneous radiologic placement of peritoneal dialysis catheters: long-term results. J Vasc Interv Radiol. 2000; 11(8): 965-970 [ Links ]
10. Abdel-Aal AK, Joshi AK, Saddekni S, Maya ID. Fluoroscopic and sonographic guidance to place peritoneal catheters: how we do it. AJR Am J Roentgenol. 2009; 192(4): 1085-1089 [ Links ]
11. Reddy C, Dybbro PE, Guest S. Fluoroscopically guided percutaneous peritoneal dialysis catheter placement: single center experience and review of the literature. Ren Fail. 2010; 32(3): 294-299 [ Links ]
12. Jacobs IG, Gray RR, Elliott DS, Grosman H. Radiologic placement of peritoneal dialysis catheters: preliminary experience. Radiology. 1992; 182(1): 251-255 [ Links ]
13. Moon JY, Song S, Jung KH, Park M, Lee SH, Ihm CG, Oh JH et al. Fluoroscopically guided peritoneal dialysis catheter placement: long-term results from a single center. Perit Dial Int. 2008; 28(2): 163-169 [ Links ]
14. Rosenthal MA, Yang PS, Liu IL, Sim JJ, Kujubu DA, Rasgon SA, et al. Comparison of outcomes of peritoneal dialysis catheters placed by the fluoroscopically guided percutaneous method versus directly visualized surgical method. J Vasc Interv Radiol. 2008; 19(8): 1202-1207 [ Links ]
15. Vaux EC, Torrie PH, Barker LC, Naik RB, Gibson MR. Percutaneous fluoroscopically guided placement of peritoneal dialysis catheters–a 10-year experience. Semin Dial. 2008; 21(5): 459-465 [ Links ]
16. Leblanc M, Ouimet D, Pichette V. Dialysate leaks in peritoneal dialysis. Semin Dial. 2001; 14(1): 50-54 [ Links ]
Joana Rego Silva, MD
Nephrology Department
Hospital Garcia de Orta;Av Torrado da Silva, 2805-267 Almada
E-mail: joanaregosilva@gmail.comtDisclosure of potential conflicts of interest: none declared.
Received for publication: Jul 15, 2018
Accepted in revised form: Sep 11, 2018


{kind=link}