











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Popliteal artery injury (PAI) is the most common cause of amputation in injured extremities1 because the popliteal artery is a true end artery with a tenuous collateral supply2.
Although uncommon overall, the incidence of PAI varies widely by setting (military vs civilian), location (urban vs rural), and predominant injury mechanism (penetrating vs blunt). Particularly, the incidence of PAI resulting from knee dislocations and knee fractures remains unclear.
Similarly, outcomes such as limb salvage rates vary widely by center and study interval, with the most favorable results being reported in modern series by high-volume civilian centers.3
The primary aim of this study was to estimate the incidence of arterial injury in patients with traumatic knee injury (specifically knee dislocation, distal femur, or proximal tibia fractures) requiring inpatient care. Secondary aims were to describe the demographics characteristics of patients with traumatic PAI, therapeutic management, amputation rates and outcomes.
Material and methods
ICD-10/ ICD-9 codes (S85.0/904.41; S83.1/836.5; S83.4; S83.5; S72,4/821.2; S82,1/823.0) were used to identify patients admitted with popliteal artery injury and/or knee trauma at our tertiary center from 1/1/2010 to 31/5/2021.
Knee dislocation was primarily defined by the ICD-10 code S83.1 and ICD-9 code 836.5. A wider definition using the combination of cruciate ligament injury (S83.5) with collateral ligament injury (S83.4) was also included. Knee fracture was defined as a proximal tibial fracture (S82.1/823.0) or a distal femoral fracture (S72.4/821.2). Fracture of patella was excluded from the definition of knee fracture.
Popliteal artery injury was identified by the ICD-10 code S85.0 and ICD-9 code 904.41
We calculate the incidence of PAI after knee trauma and using clinical and imaging records we reported the demographics characteristics of patients with traumatic PAI, therapeutic management, amputation rates and outcomes.
A statistical analysis was performed using the SPSS program version27. The categorical variables were described by frequency and percentage. Continuous variables with normal distribution were expressed through the mean and standard deviation and non-continuous variables by median and interquartile range. The normality of the distribution of variables was assessed using the Kolmogorov-Smirnov test or skewness and kurtosis.
Results
At our center from 1/1/2010 to 31/5/2021 were admitted 535 patients with knee trauma (28 with knee dislocation and 507 with fracture close to knee) and 9 patients with PAI.
Incidence
The incidence of PAI after knee trauma was 1,5%, after knee dislocation was 17,9% and after fracture close to the knee was 0,8%.
Demographics, Etiology, Other associated injuries of patients with PAI
Regarding patients with PAI, 7 (77.7 %) were male with a median age of 39.0 years.
The mechanisms of PAI were four motorcycle accidents; one bicycle accident; one work accident with heavy machinery, one fall, one running over and one iatrogenic injury (during knee arthroplasty).
Regarding associated tissue injuries, four patients (44.4%) had severe soft tissue damage, two patients(22.2%) had major nerve disruptions and two patients (22.2%) had venous injuries.
In all patients the diagnosis was made by clinical signs, confirmed by CT angiogram (6; 66%), angiography (1; 11.1%), CT angiogram and angiography (1) or surgical exploration (1)
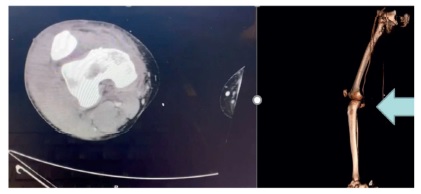
Image 1: CT angiogram and 2D reconstruction which shows a popliteal artery injury without distal arterial axis.

Treatment and outcomes
In six patients (75%), external fixator was performed before vascular restoration. In two patients (25%), revascularization was prior to orthopedic management. (The patient with iatrogenic lesion was not considered). The median ischemic time was 6.0 hours.
Regarding vascular treatment, eight patients were submitted to bypass surgery with contralateral GSV (five popliteal-popliteal bypass; two popliteal-posterior tibial bypass; one femoral - posterior tibial bypass) and one patient was treated conservatively. Mean vascular surgical time was 2.4 hours. Therapeutic fasciotomies were performed in three patients. The technique used was a two-incision four-compartment fasciotomy. No primary amputations were performed.
The median number of surgeries done per patient was 2+-1.75. Four patients were submitted to a plastic reconstructive surgery in second time.
A secondary major amputation was performed in one (11.1%) patient.
The mean hospital length of stay was 24.9 days and mortality was 0%.
During follow-up, three patients (33.3%) returned to their normal activity and six (66.7%) were limited in their daily activity.
Discussion
Patients with traumatic PAI tend to be young (with average ages in the 30s) and predominantly male (70% to 90%)4,5 which is in accordance with our serie (77.9% male with a median age of 39 years old).
The predominant cause of PAI in civilian series is blunt trauma, as we observed in our study, where only one case was caused by an iatrogenic/penetrating trauma6.
Knee dislocations are particularly at high risk of PAI, with up to 60% incidence.7 In fact, the risk of PAI after knee dislocation is higher than after knee fracture (17,9% vs 0.8% in our study, and 3,4-8,2% vs 0,2 % in Swedish registration7). Besides, knee dislocations can spontaneously reduce before emergency department presentation, but still carry the same associated risk of arterial injury and so orthopedic surgeons must be aware of this to avoid missing PAI.8 Nowadays, low-energy dislocations may be increasing since the prevalence of obesity is increasing in many countries, and severe obesity may be associated with higher risk for knee dislocation in low-energy knee injuries. However, this fact is not observed in our serie, where only one patient had a fall and 44.4% had a motorcycle accident.8
Regarding other associated injuries, significant soft tissue damage often accompanies extremity vascular trauma and the incidence reported in the literature appears close to 30%, comparing to 44.4% in our study. The presence of a significant soft tissue deficit does appear to correlate with amputation in lower extremity arterial trauma.9 The incidence of venous injury ranges between 15% and 35%, which is in accordance with our results (22.2%). There is no broad consensus as to whether such injuries should be repaired and whether failing predisposes the patient to long-term morbidity.9 For the lower extremity, most studies report nerve injury rates around 10%, which are lesser than in our serie (22.2%). The presence of a peripheral nerve injury associated with extremity vascular trauma can be difficult to detect acutely, and so may be underreported in most of the literature. Vein injuries and nerve injury does not predict amputation, even in severely injured limbs.10
Fast diagnosis and surgery decrease the ischemia period and thus the amputation rate11. Diagnosis of vascular injury in the setting of blunt trauma begins with physical examination and imaging assessment.
All patients presenting with trauma to the extremities and hard signs of arterial injury (bleeding from a penetrating wound, pulsatile hematoma, and the absence of distal pulses) should have those injuries surgically explored.12
In PAI physical examination can be misleading or initially unimpressive. A normal pulse examination may be present in 5% to 15% of patients with vascular injury. In the absence of obvious signs of vascular compromise, limb-threatening injuries are easily missed, with potentially devastating consequences. Vascular injuries include intimal tears with the majority becoming obvious in 48 to 72 hours from the time of the injury. Thus, serial clinical evaluation is justified for at least 48 hours in patients with intimal arterial lesions.13
CT angio should be considered the initial diagnostic modality of choice in stable patients with blunt or penetrating extremity trauma presenting with soft signs of extremity arterial injury, as we observed in our experience, in which 66.7% of the patients have done CT angio.13
Although vascular surgical technique may affect outcome, results are primarily dependent on early detection of vascular injury followed by immediate treatment. When repair is accomplished within 6 hours, the results are as good as those achieved with other arterial injuries.14 In our study, the median ischemic time was 6,0 hours, which should be minimized to optimize our results.
Successful management requires a multidisciplinary approach that includes the orthopaedic surgeon, vascular surgeon and plastic surgeon.
The only patient who was not operated was a patient who was not in critical ischemia (warm foot, CRT<3seg, biphasic flow in PT, and in intraoperative angiography dissection of the 2nd portion of the popliteal artery, with permeable posterior tibial and peroneal axis). In addition, the patient went into the emergency department in shock with a fractured elbow and hip and knee dislocation and therefore he already had many hours of orthopedic surgery, and so the vascular surgical team decided not to operate.
The sequence of fracture fixation and vascular repair remains controversial. Proponents of performing orthopedic intervention before vascular repair argue that bony stabilization is required to protect the vascular repair. Decreasing warm ischemia time remains the primary argument in support of performing vascular repair first. The temporary use of an intraluminal shunt was introduced to address this problem.14 In our serie, 75% of patients have done external fixation before vascular restoration due to high knee instability.
Reports of blunt popliteal arterial injuries show an incidence of graft repair between 67% and 92% which is consistent with the results of our series, in which 87.5% of patients underwent reconstruction by vein bypass. The durability of vein grafts is well documented and seems to be the best option for below knee revascularization, whereas the use of PTFE remains controversial. Conventional practice is to obtain saphenous vein grafts from uninjured extremities to preserve collateral venous drainage. This dogma is not supported by good-quality data, however, it may be appropriate to harvest conduit from an injured extremity if there is no venous injury present or if the vessel to be harvested is away from the site of injury.15 However, risk of postoperative DVT of the traumatized limb, risk of infection of the traumatized limb and increase the number of incisions in the traumatized limb to harvest a vein are all good reasons to harvest a vein in the contralateral limb.
Compartment syndrome after vascular repair is associated with high rates of limb loss.16 Lim et al1 and Frykberg et al2 have suggested implementation of prophylactic fasciotomy before arterial repair to induce restoration of the collateral circulation. However, there is no consensus regarding a prophylactic fasciotomy to improve the outcome after PAI. In our serie, fasciotomy was performed in 33.3% of the patients due to clinically apparent compartment hypertension and no prophylactic procedure were done. After 6 hours of ischemia, fasciotomies are often necessary. In our case, despite only having formally performed 3 fasciotomies, 4 of the patients had extensive soft tissue lesions and therefore already had "fasciotomies" performed by the lesions themselves.
Multidisciplinary treatment is also essential to decide which patients should be primarily amputated, which is the most difficult decision to make, since they are usually young patients. Sometimes, primary amputation is the best therapeutic option but it needs the consensus of the 3 specialties: Vascular Surgery, Plastic Surgery and Orthopedics, which need to effectively dialogue and reach a consensus. Individually, everyone thinks they are capable of solving the problem in their area of competence, but it is necessary to see the patient as a whole - this is rather a holistic approach. The Mess scale can help but it should never overlap with clinical experience.
Regarding amputation rate, our rate was lesser than the Swedish registration7 and the United States National Trauma Data Bank3 (11% vs 28% vs 14,5%, respectively). However, it’s still a high rate onsidering that it mostly affects a young and active population and only 33,3% return to a normal life. The high amputation rates seen in patients with blunt vascular injuries to the extremities can be attributed to the high-energy mechanism of such injuries and the resultant amount of damage to bone, nerve, and soft tissue, and not typically to the vascular injury itself.17 The patient undergoing secondary amputation in our serie had 7h ischemia and extensive soft tissue injury.
Conclusion
PAI is an uncommon but potentially devastating problem that carries the greatest risk of limb loss of any traumatic peripheral vascular injury.
In our experience, motorcycles accident is the leading cause of PAI.
Orthopedics surgeons must take particularly attention to knee dislocations as these lesions have an increased risk of PAI.
A multidisciplinary approach is essential to decrease ischemia time and
to promote a holistic treatment of patients with PAI.

