










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.23 no.3 Lisboa jun. 2016
https://doi.org/10.1016/j.jpge.2015.10.006
ENDOSCOPIC SNAPSHOT
Massive Gastrointestinal Bleeding from an Ectopic Varix in a Non-Cirrhotic Patient: Angiographic Approach Following Endoscopic Treatment Failure
Hemorragia Digestiva Grave por Variz Ectópica em Doente Não Cirrótico: Abordagem Angiográfica Após Falência da Terapêutica Endoscópica
Joana Carmoa,*, Susana Marquesa, Miguel Bispoa,b, Pedro Barreiroa,b, Belarmino Gonçalvesc, Adalgisa Guerrac, Pedro Pinto-Marquesb, David Serrab
a Gastroenterology Department, Hospital Egas Moniz, Centro Hospitalar de Lisboa Ocidental, Lisbon, Portugal
b Gastroenterology Department, Hospital da Luz, Lisbon, Portugal
c Radiology Department, Hospital da Luz, Lisbon, Portugal
* Corresponding author.
Keywords: Duodenum, Embolization, Therapeutic, Gastrointestinal Hemorrhage, Hemostasis, Endoscopic
Palavras-chave: Duodeno, Embolização Terapêutica, Hemorragia Gastrointestinal, Hemostase Endoscópica
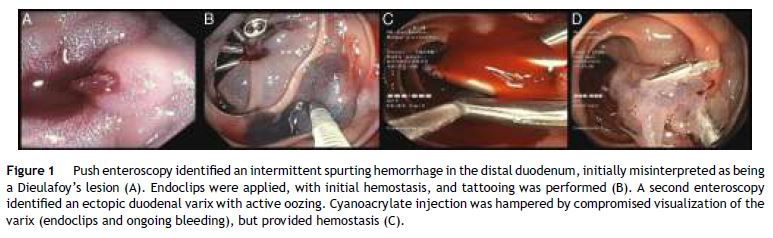
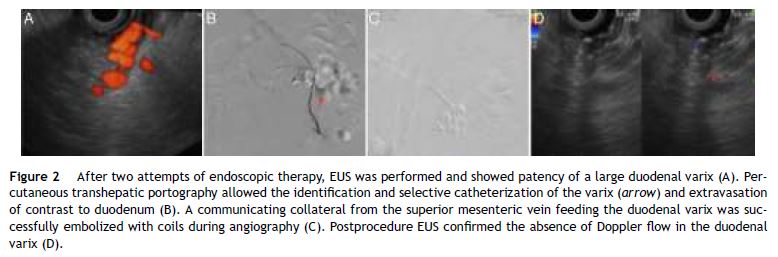
An 80-year-old male patient, with no past medical history of cirrhosis, was admitted to the emergency department of our hospital, with sudden massive hematochezia and syncope. Shortly after admission, the patient developed hemorrhagic shock, requiring substantial transfusion support (10 units of erythrocyte concentrate, 4 units of fresh frozen plasma, 1 platelet pool and 3 g of fibrinogen), renal and respiratory failure with the need of invasive mechanical ventilation. Urgent esophagogastroduodenoscopy, ileocolonoscopy and CT-angiography were inconclusive. Push enteroscopy identified an intermittent spurting hemorrhage in the third portion of the duodenum. The underlying source of bleeding was initially misinterpreted as being a Dieulafoy's lesion. Thus, endoclips were applied, with initial effective hemostasis, and tattooing was performed (Fig. 1A and B). However, severe rebleeding occurred 48 h after the procedure, with recurrence of hemodynamic instability. A second enteroscopy identified an ectopic duodenal varix with active oozing underlying the previously applied endoclips. Cyanoacrylate injection was hampered by compromised visualization of the varix (because of the previously applied endoclips and ongoing bleeding), but provided hemostasis (Fig. 1C and D). To evaluate the efficacy of cyanoacrylate injection, radial endoscopic ultrasound (EUS) was performed and showed patency (positive Doppler flow) of this large duodenal varix (Fig. 2A). In a multidisciplinary team meeting, it was decided to perform angiographic therapy, after post hoc evaluation of CT-angiography that suggested an ectopic varix with approximately 20 mm fed by a collateral of the superior mesenteric vein. Percutaneous (transhepatic) portography allowed the identification and selective catheterization of the varix. A communicating collateral from the superior mesenteric vein feeding the duodenal varix was successfully embolized during angiography with coils (Fig. 2B and C). Postprocedure EUS confirmed absence of Doppler flow in the duodenal varix (Fig. 2D). The patient's recovery was uneventful. No signs of cirrhosis or portal hypertension were documented on follow-up and the etiology of the ectopic varix remained unknown.
Ectopic varices account for 1–5% of all variceal bleeding in the setting of portal hypertension and may present as massive obscure gastrointestinal (GI) bleeding.1 Their presence should be considered in patients with portal hypertension and GI bleeding when both upper endoscopy and ileocolonoscopy are not conclusive.1 In the absence of liver disease or signs of portal hypertension this diagnosis can be challenging. The endoscopic approach to the underlying bleeding lesion was initially ineffective, stressing out the difficulty of the diagnosis and management of massive bleeding from an ectopic varix in this setting.
Although the role of EUS in GI bleeding is not well defined and not considered in the current guidelines,2 EUS can be useful in the diagnosis and management of refractory GI bleeding, particularly from vascular lesions.3,4 In this specific case, EUS was essential for the definitive diagnosis of the underlying ectopic varix and to monitor the efficacy of the delivered therapy, evaluating the permeability of the underlying bleeding varix. Therapy of ectopic varices is not well established and most authors consider endoscopic cyanoacrylate injection as the first-line therapy.1 As in the present case, angiographic techniques can be a valuable alternative in the management of bleeding vascular lesions, mainly in patients with massive obscure GI bleeding with hemodynamic instability.5
References
1. Sarin SK, Kumar CKN. Ectopic varices. Clin Liver Dis. 2012;1:167-72. [ Links ]
2. Barkun AN, Bardou M, Kuipers EJ, Sung J, Hunt RH, Martel M, et al. International Consensus Recommendations on the management of patients with nonvariceal upper gastrointestinal bleeding. Ann Intern Med. 2010;152:101-13. [ Links ]
3. Vazquez-Sequeiros E, Olcina J. Endoscopic ultrasound guided vascular access and therapy: a promising indication. World J Gastrointest Endosc. 2010;2:198-202. [ Links ]
4. Romero-Castro R, Ellrichmann M, Ortiz-Moyano C, Subtin-Inigo JC, Junquera-Florez F, Gornals JB, et al. EUS-guided coil versus cyanoacrylate therapy for the treatment of gastric varices: a multicenter study (with videos). Gastrointest Endosc. 2013;78:711-21. [ Links ]
5. Fisher L, Krinsky ML, Anderson MA, Appalaneni V, Banerjee S, Ben-Menachem T, et al. The role of endoscopy in the management of obscure GI bleeding. Gastrointest Endosc. 2010;72:471-9. [ Links ]
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Disclosures
All authors have approved the manuscript and agree with its submission to GE – Portuguese Journal of Gastroenterology. All authors have nothing to disclose and there are no funding to declare.
Conflicts of interest
The authors have no conflicts of interest to declare.
* Corresponding author.
E-mail address: joanavcarmo@gmail.com (J. Carmo).
Received 14 August 2015; accepted 25 October 2015


{kind=link}
{kind=link}