Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Intragastric balloon is a temporary nonsurgical treatment for weight loss [1, 2]. The standard routine for its removal consists of: (i) puncturing with a needle held in the aspirator; (ii) pushing the needle inside the balloon, leaving the catheter inside; (iii) connecting the catheter to a vacuum drainage device, and then aspiring the entire balloon content; (iv) removing the collapsed balloon with a wire grasper. We hereby present a difficult intragastric balloon retrieval using a different technique.
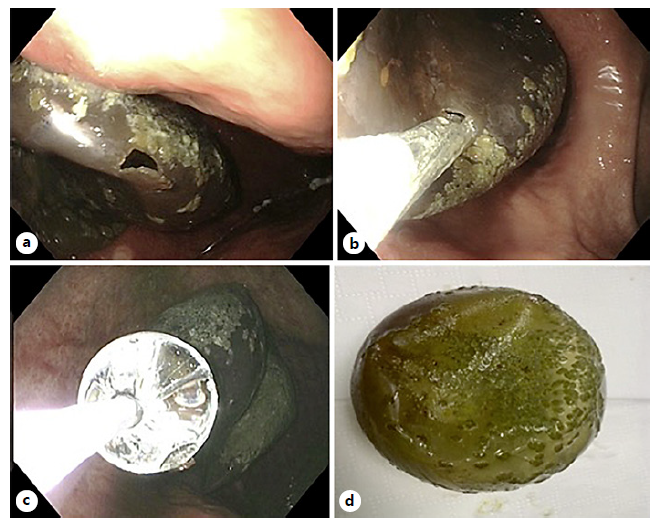
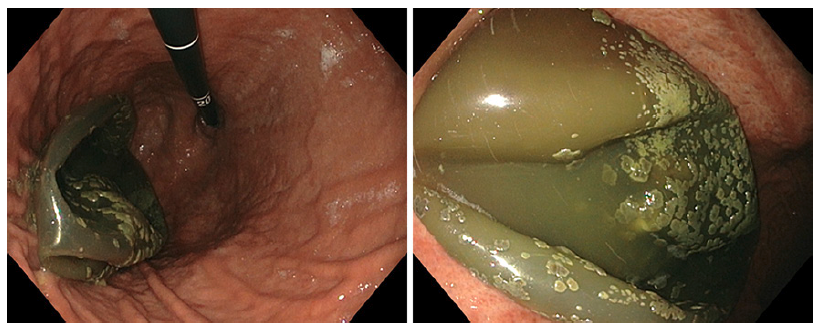
A 39-year-old woman, with no significant medical history but obesity, was referred to our center after an unsuccessful Bioenteric Intragastric Balloon (BIB) retrieval. The balloon had been placed 5 months earlier and since then the patient had lost 8 Kg. On the first retrieval attempt, the aspiration of the BIB content with a standard BIB kit (Apollo Endosurgery, consisting of a wire grasper removal instrument and a needle aspirator) had not resulted in its full collapse. Therefore, the balloon could not be removed, as it did not pass the esophagogastric junction. At our unit, under propofol sedation, a second attempt to fully aspirate the balloon with the same system was ineffective, as the surface of the balloon was pliable (Fig. 1). While mobilizing the BIB with the two-prong grasper device, a small hole was accidentally made (Fig. 2a); this allowed the needle to be inserted and the suctioning of some fluid. However, it was not possible to fully aspirate the balloon. Therefore, to promote passive emptying, we decided to enlarge the hole with a through-the-scope balloon dilator (18/19/20 mm, EndoFlex® Ref. 34118PRO; Fig. 2b, c). This allowed the volume of the balloon to be reduced, which was then gently retrieved with the two-prong grasper (Fig. 2d). Re-examination of the stomach and esophagus was unremarkable, and the women was asymptomatic afterwards. Balloon retrieval may be a challenging task, especially when it is maintained longer than the recommended 6 months [3]. Some[ non-standard retrieval techniques have already been described, such as the use of a larger needle with a stronger suction device, the use of a snare around the end of the endoscope, or spraying vegetable oil over the balloon to ease balloon passage [4]. A procedure identical to ours was described by a Canadian group, who used a through-the-scope balloon dilator to allow intragastric balloon de-compression. The balloon was then removed through an overtube, using a snare [5].
.