











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkA 67-year-old female, with no relevant past medical history, underwent a screening upper endoscopy that revealed a 12 mm subepithelial lesion in the anterior face of the duodenal bulb (Fig. 1a). Biopsies were performed and revealed a well-differentiated neuroendocrine tumor (NET G1). Endoscopic ultrasound confirmed the presence of a hypoechoic lesion with 13 × 7 mm in the submucosa and no lymph node metastasis was detected. Abdominal computerized tomography and somatostatin receptor scintigraphy revealed no evidence of extra duodenal disease. After a multidisciplinary discussion, endoscopic mucosal resection (EMR) using band ligation was decided.
A conventional single-channel endoscope (GIF-HQ190; Olympus Medical Systems, Tokyo, Japan) was used for the procedure. Marking of the borders of the lesion was performed with argon plasma coagulation, followed by sub-mucosal injection with saline, diluted adrenaline, blue methylene, and colloid solution (Fig. 1b). This was per-formed to reduce the risk of muscle injury during resection. The Captivator TM EMR Device (Boston Scientific) was used to perform band ligation. Several attempts of suction of the lesion into the distal cap were done to create a pseudo polyp and to achieve an adequate aspiration of the lesion. The band was correctly deployed (Fig. 1c). Then, the underwater technique was used to assist in the correct positioning of the snare. The snare was placed below the band, and hot snare resection was performed using a blended electrosurgical current (Fig. 1d). The lesion was removed by aspirating it into a cap. Inspection of the resection bed revealed no signs of muscular injury or other complications (Fig. 1e). The mucosal defect was closed using 4 through-the-scope clips (Fig. 1f). The histopathology report confirmed complete curative resection of the lesion (NET G1, pT1NxR0). The patient remains well in the follow-up, with no evidence of disease recurrence.
Duodenal NETs comprise 15% of all gastrointestinal NETs [1]. They are generally small, with a mean size of 1.2-1.5 cm, and usually limited to the submucosa or mucosa. All duodenal NETs should be removed, unless in the presence of distant metastases or of medical conditions that markedly limit life expectancy [2]. Small tumors can be locally resected by endoscopy, and en bloc resection is recommended [3]. However, studies on the best resection
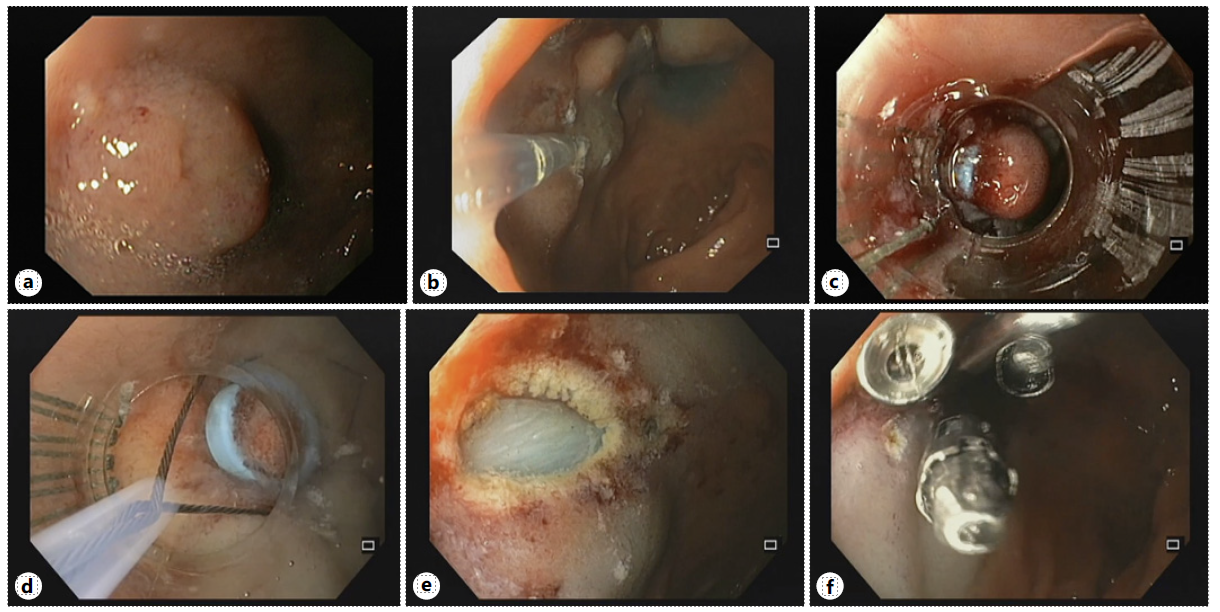
Fig. 1 a Duodenal NET. b Saline solution was injected in the submucosal layer. c The tumor was aspirated into the ligator device, followed by deployment of the elastic band. d Hot snare resection was performed below the band, using the underwater technique. e The lesion was completely removed. f The mucosal defect was closed using through-the-scope clips.
methods are lacking. Conventional EMR is occasionally associated with margin involvement and crush injury of the resected specimens, which leads to difficulty in pathological evaluation [4]. On the other hand, endoscopic submucosal dissection is technically difficult and carries a high risk of complications [5]. Endoscopic full-thickness resection (EFTR) is a minimally invasive procedure that allows for potentially curative treatment in local disease. Although several studies have reported consistent negative margins, there are limited data regarding the use of EFTR for duodenal NETs [6]. Recently, underwater EMR has also been applied for the management of these lesions, with some authors describing an en bloc resection and complete resection rates of 100%, and no complications [7]. Although the efficacy of underwater-assisted resection cannot be fully demonstrated with just a few case reports, it may rep-resent a potential alternative endoscopic approach.
This case highlights the role of EMR using band ligation as an effective, safer, and faster technique compared with conventional EMR, endoscopic submucosal dissection, and EFTR for the treatment of duodenal NETs that are confined to the submucosal layer without metastasis. In fact, this is a simple procedure that enables easy and complete resection of these tumors, without complications [8].

