










Serviços Personalizados
Journal

Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
 Citado por SciELO
Citado por SciELO Links relacionados
 Similares em
SciELO
Similares em
SciELO Compartilhar

 Permalink
PermalinkPortuguese Journal of Public Health
versão impressa ISSN 2504-3137versão On-line ISSN 2504-3145
Port J Public Health vol.35 no.3 Lisboa 2017
https://doi.org/10.1159/000488074
RESEARCH ARTICLE
Sodium and Potassium Content of Meals Served in University Canteens
Teor de sódio e potássio em refeições servidas em cantinas universitárias
Maria Inês Barbosa a Alexandra Fernandes a Carla Gonçalves a Maria João Pena ab Patrícia Padrãoac Olívia Pinhoad Pedro Moreira ace
a Faculdade de Ciências da Nutrição e Alimentação da Universidade do Porto, Porto, Portugal
b Faculdade de Medicina, Universidade do Porto, Porto, Portugal
c EPIUnit – Instituto de Saúde Pública, Universidade do Porto, Porto, Portugal
d LAQV/REQUIMTE, Universidade do Porto, Porto, Portugal
eCentro de Atividade Física, Saúde e Lazer, Universidade do Porto, Porto, Portugal
ABSTRACT
A high sodium intake is associated with high blood pressure, an important risk factor for noncommunicable diseases (NCDs). In contrast, the ingestion of high levels of potassium counteracts this negative effect of high sodium intake on blood pressure, thus reducing the sodium-to-potassium ratio. The aim of this work was to determine the sodium and potassium content of meals served in university canteens in Portugal. The analysis included 35 samples of soup and 35 samples of main dish collected at 5 random days from a total of 7 university canteens. The samples were analyzed for sodium and potassium by atomic emission spectrometry technique. On average, a meal (soup and main dish) had a sodium content of 1,069.4 mg (mean sodium content was 671.4 ± 374.5 mg/portion in the main dish and 398.0 ± 153.0 mg/portion in the soup) and a potassium content of 1,004 mg (mean potassium content was 731.4 ± 385.9 mg/serving in the main dish and 272.6 ± 272.6 mg/serving in the soup). Our results revealed that with a single university meal, students can reach 53% of the maximum daily value recommended for sodium and 27% of the minimum daily value recommended for potassium. An investment to decrease sodium and increase potassium in meals served is imperative in order to prevent NCDs.
Keywords: Sodium Potassium Meals University canteens Atomic emission spectrometry verified
RESUMO
Uma elevada ingestão de sódio está associada à hipertensão, um importante fator de risco para doenças crónicas não transmissíveis (DCNT). Em contraste, a ingestão de níveis elevados de potássio contrabalança esse efeito negativo da elevada ingestão de sódio na pressão arterial, reduzindo, assim, a relação sódio/potássio. O objetivo deste trabalho foi determinar o teor de sódio e potássio de refeições servidas em cantinas universitárias em Portugal. A análise incluiu 35 amostras de sopa e 35 amostras de prato principal recolhidas em 5 dias aleatórios de um total de 7 cantinas universitárias. As amostras foram analisadas para sódio e potássio pela técnica de espectroscopia de emissão atómica. Uma refeição (sopa e prato principal) apresentou em média um teor de sódio de 1.069,4 mg (teor médio de sódio foi 671,4 ± 374,5 mg/porção no prato principal e 398,0 ± 153,0 mg/porção na sopa) e um teor de potássio de 1.004 mg (teor médio de potássio foi de 731,4 ± 385,9 mg/porção no prato principal e 272,6 ± 272,6 mg/porção na sopa). Os resultados mostraram que, com uma única refeição universitária, os alunos podem atingir 53% do valor máximo diário recomendado para o sódio e 27% do valor mínimo diário recomendado para o potássio. Um investimento para diminuir o sódio e aumentar o potássio nas refeições servidas é imperativo para prevenir as DCNT.
Palavras-chave: Sódio · Potássio · Refeições · Cantinas universitárias · Espectroscopia emissão atómica
Introduction
Noncommunicable diseases (NCDs) are the leading cause of death globally 1. In Portugal, NCDs account for about 86% of all deaths (2 ) and the prevalence of hypertension in adults is 42.2% (3 ). Several population-based studies worldwide have documented the association between high sodium intake and hypertension 4.
The salt from processed foods and the salt added to food during the cooking process are the main sources of sodium intake 5. Besides the increase of blood pressure, high salt intake is associated with an increased risk of gastric cancer (6 , 7 ), development of cardiovascular damages 8, increased left ventricular mass (9 , 10 ), occurrence of cerebrovascular disease 11, and increased arterial stiffness (12 , 13 ).
It was documented that a 5-gram reduction in daily salt intake by the general population could prevent one and a quarter million deaths from stroke and almost three million deaths from cardiovascular disease each year 14. On the opposite, potassium intake can mitigate the negative effects of high sodium intake 15, namely because of its antihypertensive effects. It has been described that potassium decreases intravascular volume, partly through decreased sodium reabsorption, i.e., increased urinary sodium excretion 16. Likewise, potassium is an essential nutrient needed for maintenance of total body fluid volume, acid and electrolyte balance, and normal cell function 17.
A low potassium intake has been reported as a major public health problem in the USA, with negative effects on cardiovascular disease, renal stone development, and bone mineral density (15 , 18 ). On the other hand, if recommendations for both sodium and potassium are achieved, the sodium-to-potassium ratio should be close to 1.0 mmol/mmol (0.59 mg/mg), which may be reached with an adequate intake of fruit and vegetables 19. High dietary sodium-to-potassium ratios have been linked to a higher risk of NCDs, including coronary heart disease and stroke 20. Therefore, potassium is seen as one of the key nutrients to prevent NCDs 21.
Potassium is mostly found in a variety of unrefined foods, particularly in fruit and vegetables. Food processing reduces the amount of potassium in many food products, so a diet rich in processed foods and poor in fresh fruit and vegetables is often associated with a low potassium diet 22.
The WHO established recommendations for both sodium and potassium in order to reduce blood pressure and risk of cardiovascular disease, stroke, and coronary heart disease in adults. The WHO recommends a maximum daily intake of 2,000 mg of sodium (5 g/day of salt) (23 ) and suggested a potassium intake of at least 3,510 mg/day for the adult population 21.
The canteens are the place chosen by university students for eating most meals out of home, and are also a privileged place to promote healthy eating habits (24 , 25 ). The aim of this study was to determine sodium and potassium content in university canteen meals.
Material and Methods
Sample Collection
The samples were collected at 7 canteens from a Portuguese university, on 5 random days, between February and May 2015. One sample of soup and one sample of main dish were collected at each visit at the canteens. As the units presented 5 types of main dishes each day (meat, fish, vegetarian, and diet), on the fifth day of sample collection, a type of main dish was repeated, randomly chosen. The final sample consisted of 35 soups and 35 main dishes.
The samples were collected at lunchtime. Samples were weighed in the kitchen and each component was weighed separately in the case of the main dish (e.g., first rice was weighed, then salad, then meat, etc.). Soup and main dishes were transported to the laboratory in separate hermetic plastic bags in a refrigerated cooler box.
The samples were prepared on the same day of collection and only the edible part was considered after deboning fish and meat. Soups were homogenized with a hand blender (Electric Co 450 W®), while the main dish components were mixed up with an electric food chopper (Moulinex 700 W®) into a homogenous mass of food. The homogenized mass obtained from samples was distributed on PTFE 60 mL containers and stored in a freezer (–18°C) until it was used.
Chemical Analysis
Sodium and potassium content was determined by atomic emission spectrometry (AES).
Reagents and Standard Solutions
All reagents were of analytical grade and solutions were prepared with deionized water, obtained from Seralpur PRO 90 CN and Seradest LFM 20 water purification system. For the analysis of sodium by AES, sodium standard solution (1,000 ppm) was supplied by JenWay (England), potassium standard solution (1,000 ppm) was supplied by JenWay (England), and nitric acid 70% (HNO3) was purchased from Sigma (USA). Solutions used for calibration curves were stored in the refrigerator. Standard solutions were prepared daily from a 1,000 ppm stock solution, with the following concentrations: 0.2, 0.5, 1.0, 2.5, and 5.0 ppm. Standard solutions were read on the photometer before sample readings and a standard solution was read for verification every 10 readings of samples. All PTFE materials were cleaned, bathed in 10% HNO3 overnight, and rinsed twice with double distilled water.
Analysis by AES
The samples were analyzed by AES by a flame photometer (PFP7, JenWay, UK). The samples were analyzed in duplicate, with three readings of each extraction. A portion of 2 g of the sample was weighed (KERN ALS 120-4®, Germany) and then 2 mL of HNO3 were added. The mixture was then manually shaken carefully every 10 min for 90 min. After this time, the mixture was filled up with deionized water to 45 mL and homogenized using an Ultraturrax (Ystral®, The Netherlands) and shaken vigorously every 5 min for 30 min. Then, 12 mL of solution centrifuged (Labofuge 6000, Haerus, Germany) at 4,000 rpm for 10 min. Finally, 1 mL of supernatant was diluted up to 40 mL and a reading was taken.
Statistical Analysis
The analysis of the data was performed using the Statistics® SPSS software (version 22.0) for Microsoft Windows®. The data were presented in mg per 100 g of meal and in mg per serving, as mean and standard deviation (mean ± SD). Each canteen was assigned an encoding letter (A through G).
The Kolmogorov-Smirnov test was used to test the normality of the variables, presented as mean ± SD. One-way ANOVA test was performed to verify the differences in the content of both minerals between the units (Table 1) and between different types of main dish (Table 2). A p value < 0.05 was considered as significant.
Results
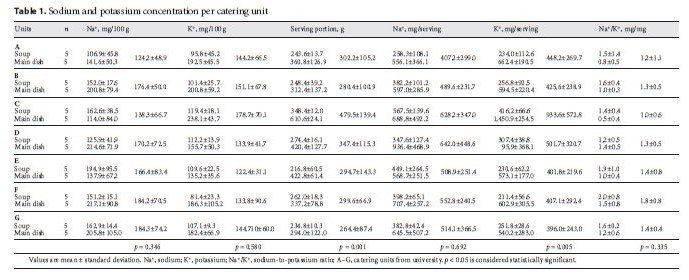
Results are organized in two tables. Table 1 shows the analysis for each canteen. The sodium and potassium concentration (mg/100 g), sodium-to-potassium ratio (mg/mg), size of serving portion (g), and the sodium and potassium concentration per serving were expressed. These values are presented for soup, main dish, and average meal served in each unit (soup and main dish). In this table, it is seen that the serving portion varied significantly between catering units (p = 0.001).
Regarding sodium concentration (mg/100 g) and sodium concentration per serving (mg/serving), no statistically significant differences between catering units were found (p = 0.692). However, it was noted that the sodium content in the average number of meals (soup + main dish) in each unit ranged between 407.2 and 642 mg/serving. For potassium concentration (mg/100 g), no statistically significant differences between catering units were found (p = 0.580), but when the average concentration of potassium per serving (mg/serving) was considered, unit C had the highest concentration with 933.6 ± 572.8 mg, and the unit that had fewer potassium per serving was unit G with 396.0 ± 243.0 mg (p = 0.005). Sodium-to-potassium ratio did not have statistically significant differences between catering units, and varied between 1.0 ± 0.6 (unit C) and 1.8 ± 0.8 (unit F).
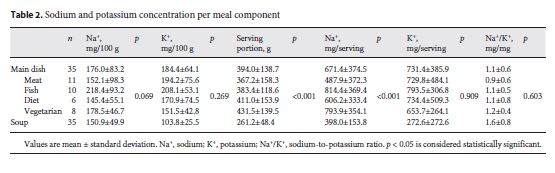
Table 2 shows the average values for the main dishes and soups, and also shows sodium, potassium, and sodium-to-potassium ratio values in each type of main dish (meat, fish, diet, and vegetarian). The sodium content of the main dish served in the units was on average 176.0 ± 83.2 mg/100 g. Regarding the sodium content in an average serving of main dish, the mean was 671.4 ± 374.5 mg/serving (corresponding to 1.8 ± 1.0 g salt/serving), without statistically significant differences in sodium (mg/100 g) between different types of main dish (p = 0.069). Nonetheless, as the size of the serving portion of a meal varied between different types of main dish (p < 0.001), it was found that fish and vegetarian dishes were the ones with higher sodium content representing 814.4 ± 369.4 mg/serving and 793.9 ± 354.1 mg/serving, respectively.
With regard to soups, the mean sodium content was 150.9 ± 49.9 mg/100 g and 398.0 ± 153.8 mg/serving (corresponding to 1.0 ± 0.4 g salt/serving). The potassium content of soups was, on average, 103.8 ± 25.5 mg/100 g, while the main dish was 184.4 ± 64.1 mg/100 g. There were no statistically significant differences between the different types of main dish. We verified a sodium-to-potassium ratio of 1.1 in main dish and 1.6 in soup. No statistically significant differences were found between different types of main dish.
Discussion
The main result of this study was the high sodium and the low potassium content, compared to the recommended daily intake, that were found in the components of the meals served in university canteens.
High sodium intake by populations around the world and particularly in Portugal has been the subject of much attention by experts in the field of nutrition and cardiovascular health 26, especially when it comes to eating out of home 27.
The results showed that sodium content in the main dish was, on average, 671.4 ± 374.5 mg/serving and that fish and vegetarian dishes were those with higher sodium content by serving (814.4 ± 369 4 mg in fish dish and 793.9 ± 354.1 mg in vegetarian dish; p < 0.001).
The fish dishes may be the less preferred by university students 28 and eventually, food handlers may feel the need to add more salt in order to make the fish dishes more palatable and consequently more consumed.
Vegetarian dishes usually have vegetables in its composition, whose sodium contribution is virtually nonexistent 29. However, pickled foods (seitan, soy, and tofu) and other products (e.g., puff pastry, salty cheeses) that are widely used in these main dishes, have a fairly high sodium contribution (30 , 31 ). Given the intrinsic sodium content of these foods, the addition of salt during cooking in such dishes should be reconsidered.
Soup had an average of 398.0 ± 153.8 mg of sodium per serving. The study of Gonçalves et al. 32, held in Portugal, which compared the sodium content of soups before and after adding salt, showed that the sodium content of soups was significantly higher after salt addition. This suggests that the main factor responsible for the sodium levels found in soups is the addition of salt during the cooking process (over 90% of sodium) 32. Our results are similar to the results of previous studies (33 , 34 ), however with slightly lower sodium content.
Main dish showed higher sodium content than soup (Table 2), probably due to the fact that intrinsic sodium present in foods, such as meat and fish, is higher than sodium intrinsically present in vegetables used for soups 29, other reason could be that the main dishes are more suitable to use condiments (e.g., broths, pre-prepared sauces) which are very rich in sodium (29 , 35 ), and finally because the level of salt added in a main dish during cooking could be higher than in soups.
On average, one meal composed of soup and main dish had a sodium content of 1,069.4 mg/serving (corresponding to 2.8 g of salt/serving). Since the WHO recommends a maximum daily intake of 2,000 mg of sodium (5 g of salt), the sodium content of one meal reached about 53% of the recommended daily intake.
During the visits to the catering units, it was found that the addition of salt was under the responsibility of the chef responsible for seasoning the meals and that the amount of salt added was done by instinct. The amount of added salt is influenced by the taste of the chef; however, many food handlers recognize that they do not taste foods before adding salt 36.
Reducing the addition of salt is controversial, and some people consider that salt is a single ingredient, impossible to replace, being the one that gives flavor to food 37. A study with Portuguese food handlers showed that many of the food handlers were aware of the recommended salt intake values and health problems associated with excessive salt intake. They were sensitive to reducing the salt content of foods produced but referred that the greatest difficulties in salt reduction were the opinion and knowledge of consumers and food handlers 36. Thus, it is important to educate consumers and food handlers, so that actions to reduce the amount of salt added to meals start to be effective.
The replacement of salt with herbs and spices is a possible strategy to gradually reduce the salt added to meals. Herbs may positively influence health, either by giving flavor, aroma, and color to meals or by offering beneficial properties for human health 38.
A strategy that could decrease the high variability among sodium content between canteens could be the use of a standard measure of salt to be added to each component of the meal that respects the daily sodium recommendations. Another way could be the implementation of a fast and easy device that informs the food handler about the amount of salt present in food.
Salt reduction must be done without causing significant changes in the salt perception and hedonic perception of consumers. In complex dishes (where all ingredients contribute to the flavor, such as soups), sodium content may be reduced by about 30% without causing significant changes in the salt perception (39 , 40 ). This suggests that a reduction of added salt in this order of magnitude may not interfere with the sensory level, and it is one possible measure to be taken to fight the high sodium levels.
Regarding potassium levels, main dishes had higher potassium values than soup (mg/100 g), which was unexpected, because Portuguese soups are considered comfort food rich in boiled vegetables. Soup is often described as an important source of vitamins and minerals, such as potassium 41. The role of the potassium supplier depends on a food matrix rich in vegetables and, in some cases, pulses.
The average potassium values found in the analyzed soups were lower than the potassium content of soups described in the Portuguese food composition table 29, suggesting that our soups could have less vegetables and pulses in their composition. A study analyzing 14 soups of scholar meals 34 reported a higher potassium content than our study, which supports the supposition that soups analyzed in our study had an insufficient amount of vegetables. Main dishes had a higher potassium content than soups, maybe due to the presence of animal products (meat and fish), which were important sources of potassium in addition to the vegetables also served in the main dish.
It is also worth noting that in some units, the sodium-to-potassium ratio of soups was almost twice the ideal ratio, which is supposed to be approximately 1.0, which confirms the idea that soups had much more sodium and less potassium than they should have. Also, the ratio was higher in soup than it was in main dishes.
Our findings revealed an amount of 1,004 mg of potassium, considering soup and main dish, which corresponds to 27% of the WHO daily intake recommendation for potassium. A study addressing the eating habits of Portuguese university students showed a low intake of fruit and vegetables, and that many of the students did not eat soup daily 42. Therefore, the amount of potassium ingested by students can be significantly lower than potassium available in meals if they do not eat soup.
The results obtained emphasize the need to consolidate or increase potassium availability in these meals, in order to promote potassium intake in the population, through foods rich in this mineral. The best way to increase potassium intake is to privilege the consumption of fruit and vegetables 43, which itself may have other beneficial effects on health given its content in micronutrients, fiber, and antioxidants (43 , 44 ), without significantly increasing the energy intake or undesirable nutrients.
The amount of vegetables added to the soup and the main dish could be more generous, and the portions served more homogeneous among the units in order to increase potassium availability. Food education sessions for consumers of the canteens could also be an improvement in order to sensitize them to the importance of the consumption of vegetables, pulses, and fruit and consequently encourage the consumption of the various components of the meal. Conducting training sessions for professionals of the units reinforces the principles mentioned above.
Conclusion
In conclusion, the average amount of sodium of a meal served in university canteens corresponds to 53% of the daily sodium intake recommendation, whereas potassium levels found in these meals correspond to 27% of the daily potassium intake recommendation. Consumers of meals in university canteens can easily exceed the maximum daily intake for sodium. On the other hand, the potassium recommendation could be difficult to achieve if consumers do not eat soup. An investment by catering companies and social services in training their human resources is imperative in order to increase their awareness of the issue of decreasing salt addition and increasing vegetable availability.
Acknowledgments
We thank especially the Social Services of the university for the authorization of the study.
Received: March 16, 2016
Accepted: February 7, 2018
REFERENCES
1 World Health Organization: Global Status Report on Noncommunicable Diseases. Geneva: WHO; 2010. [ Links ]
2 World Health Organization: Noncommunicable Diseases (NCD): Country Profiles. Geneva: WHO; 2014. [ Links ]
3 Polonia J, Martins L, Pinto F, Nazare J: Prevalence, awareness, treatment and control of hypertension and salt intake in Portugal: changes over a decade. The PHYSA study. J Hypertens 2014; 32: 1211–1221.10.1097/HJH.000000000000016224675681
4 Reddy V, Sridhar A, Machado RF, Chen J: High sodium causes hypertension: evidence from clinical trials and animal experiments. J Integr Med 2015; 13: 1–8.10.1016/S2095-4964(15)60155-825609366
5 The Caroline Walker Trust: Eating Well for Looked After Children and Young People: Nutritional and Practical Guidelines: Report of an Expert Working Group. Herts, UK: The Caroline Walker Trust; 2001. [ Links ]
6 Sugimura T, Wakabayashi K: Gastric carcinogenesis: diet as a causative factor. Med Oncol Tumor Pharmacother 1990; 7: 87–92.2232942
7 Tsugane S: Salt, salted food intake, and risk of gastric cancer: epidemiologic evidence. Cancer Sci 2005; 96: 1–6.10.1111/j.1349-7006.2005.00006.x15649247
8 Strazzullo P: Salt-sensitivity, hypertension and cardiovascular ageing: broadening our view without missing the point. J Hypertens 2002; 20: 561–563.10.1097/00004872-200204000-0000211910280
9 Messerli FH, Aepfelbacher FC: Hypertension and left-ventricular hypertrophy. Cardiol Clin 1995; 13: 549–557.8565018
10 Schmieder RE, Messerli FH, Ruddel H, Garavaglia GG, Grube E, Nunez BD, et al: Sodium intake modulates left ventricular hypertrophy in essential hypertension. J Hypertens Suppl 1988; 6:S148–S150.2977158
11 Perry IJ: Dietary salt intake and cerebrovascular damage. Nutrit Metab Cardiovasc Dis 2000; 10: 229–235.11079261
12 Polónia J, Maldonado J, Ramos R, Bertoquini S, Duro M, Almeida C, et al: Determinação do consumo de sal numa amostra da população portuguesa adulta pela excreção urinária de sódio: sua relação com rigidez arterial. Rev Port Cardiol 2006; 25: 801–817.17100171
13 Gates PE, Tanaka H, Hiatt WR, Seals DR: Dietary sodium restriction rapidly improves large elastic artery compliance in older adults with systolic hypertension. Hypertension 2004; 44: 35–41.10.1161/01.HYP.0000132767.74476.6415173128
14 Strazzullo P, D’Elia L, Kandala NB, Cappuccio FP: Salt intake, stroke, and cardiovascular disease: meta-analysis of prospective studies. BMJ 2009; 339:b4567.10.1136/bmj.b456719934192
15 Whelton PK, He J, Cutler JA, Brancati FL, Appel LJ, Follmann D, et al: Effects of oral potassium on blood pressure: meta-analysis of randomized controlled clinical trials. JAMA 1997; 277: 1624–1632.10.1001/jama.1997.035404400580339168293
16 Weaver CM: Potassium and health. Adv Nutr 2013; 4: 368s–377s.10.3945/an.112.00353323674806
17 Young B: Role of Potassium in Preventive Cardiovascular Medicine. Boston: Kluwer Academic Publishers; 2001. [ Links ]
18 United States Department of Agriculture. Department of Health and Human Services. Dietary Guidelines Advisory Committee. Scientific Report of the 2015 Dietary Guidelines Advisory Committee. Washington, DC: USDA. HHS; 2015. [ Links ]
19 World Health Organization: Diet, Nutrition and the Prevention of Chronic Diseases. Geneva: WHO; 2003 (Technical report series; 916).
20 Yang Q, Liu T, Kuklina EV, Flanders WD, Hong Y, Gillespie C, et al: Sodium and potassium intake and mortality among US adults: prospective data from the Third National Health and Nutrition Examination Survey. Arch Intern Med 2011; 171: 1183–1191.10.1001/archinternmed.2011.25721747015
21 World Health Organization: Guideline: Potassium Intake for Adults and Children. Geneva: WHO; 2012. [ Links ]
22 Webster JL, Dunford EK, Neal BC: A systematic survey of the sodium contents of processed foods. Am J Clin Nutr 2010; 91: 413–420.10.3945/ajcn.2009.2868819955402
23 World Health Organization: Guideline: Sodium Intake for Adults and Children. Geneva: WHO; 2012. [ Links ]
24 Lachat CK, Huybregts LF, Roberfroid DA, Van Camp J, Remaut-De Winter AM, Debruyne P, et al: Nutritional profile of foods offered and consumed in a Belgian university canteen. Public Health Nutr 2009; 12: 122–128.10.1017/S136898000800204818416870
25 Fernandez Torres A, Moreno-Rojas R, Camara Martos F: Nutritional content of foods offered and consumed in a Spanish university canteen. Nutr Hosp 2015; 31: 1302–1308.10.3305/nh.2015.31.3.800625726226
26 He FJ, MacGregor GA: A comprehensive review on salt and health and current experience of worldwide salt reduction programmes. J Hum Hypertens 2009; 23: 363–384.10.1038/jhh.2008.144)19110538
27 Lachat C, Nago E, Verstraeten R, Roberfroid D, Van Camp J, Kolsteren P: Eating out of home and its association with dietary intake: a systematic review of the evidence. Obes Rev 2012; 13: 329–346.10.1111/j.1467-789X.2011.00953.x22106948
28 Martinez Alvarez JR, Garcia Alcon R, Villarino Marin A, Marrodan Serrano MD, Serrano Morago L: Eating habits and preferences among the student population of the Complutense University of Madrid. Public Health Nutr 2015; 18: 2654–2659.10.1017/S136898001500002625683651
29 Portugal. Ministério da Saúde. Instituto Nacional de Saúde Dr. Ricardo Jorge. Centro de Segurança Alimentar e Nutrição. Tabela da composição de alimentos. Lisboa: INSA; 2007. [ Links ]
30 Weaver CM, Dwyer J, Fulgoni VL 3rd, King JC, Leveille GA, MacDonald RS, et al: Processed foods: contributions to nutrition. Am J Clin Nutr 2014; 99: 1525–1542.10.3945/ajcn.114.08928424760975
31 Dwyer JT, Fulgoni VL 3rd, Clemens RA, Schmidt DB, Freedman MR: Is “processed” a four-letter word? The role of processed foods in achieving dietary guidelines and nutrient recommendations. Adv Nutr 2012; 3: 536–548.10.3945/an.111.00090122797990
32 Gonçalves C, Silva G, Pinho O, Camelo S, Amaro L, Teixeira VH, et al: Sodium Content in Vegetable Soups Prepared outside the Home: Identifying the Problem. Occupational Safety Hygiene SHO Series. 2012. [ Links ]
33 Reis AT, Toscano MM, Meister MC: Sal em sopas. Segurança e Qualidade Alimentar 2008; 4: 54–55.
34 Martins BM: Quantificação de sódio e potássio em sopas de ementas escolares do 1°, 2° e 3° ciclos. Universidade do Porto; 2012. [ Links ]
35 Wu Leung WT, Rauanheimo Butrum R, Huang Chang F, Narayana Rao M, Polacchi W: Food Composition Table for Use in East Asia. Rome (Italy): FAO and US Department of Health, Education, and Welfare; 1972. [ Links ]
36 Gonçalves C, Pinho O, Padrão P, Santos C, Abreu S, Moreira P: Knowledge and practices related to added salt in meals by food handlers. Nutrícias (online) 2014; 21: 14–17.
37 Bourdain A: Kitchen Confidential: Adventures in the Culinary Underbelly. New York, NY: Bloomsbury Publishing; 2007. [ Links ]
38 Tapsell LC, Hemphill I, Cobiac L, Patch CS, Sullivan DR, Fenech M, et al: Health benefits of herbs and spices: the past, the present, the future. Med J Aust 2006; 185(4 suppl):S4–S24.17022438
39 Malherbe M, Walsh CM, Van der Merwe CA: Consumer acceptability and salt perception of food with a reduced sodium content. J Fam Ecol Consum Sci 2003; 31: 12–20.
40 Gonçalves C, Monteiro S, Padrao P, Rocha A, Abreu S, Pinho O, et al: Salt reduction in vegetable soup does not affect saltiness intensity and liking in the elderly and children. Food Nutr Res 2014; 58: 1–7.10.3402/fnr.v58.2482525317121
41 Associação Portuguesa de Nutricionistas. Sopas: mais que um alimento, são um prato de saúde. Lisboa: APN; 2013. [ Links ]
42 Martins ML: Hábitos alimentares de estudantes universitários. Porto: Faculdade de Ciências da Nutrição e Alimentação da Universidade do Porto; 2009. Trabalho de investigação.
43 He FJ, MacGregor GA: Beneficial effects of potassium on human health. Physiol Plant 2008; 133: 725–735.10.1111/j.1399-3054.2007.01033.x18724413
44Hu D, Huang J, Wang Y, Zhang D, Qu Y: Fruits and vegetables consumption and risk of stroke: a meta-analysis of prospective cohort studies. Stroke 2014; 45: 1613–1619.10.1161/STROKEAHA.114.00483624811336t

