











 (pdf)
(pdf)




 SciELO
SciELO  SciELO
SciELO 
 Permalink
Permalink
Introduction
The abdominal aortic aneurysm (AAA) corresponds to a dilation ≥ 3.0cm in the anteroposterior or transverse planes of the abdominal aorta, mainly affecting men aged ≥ 65 years, especially those who had ever smoked. Its growth is silent, and, in most cases, it only manifests itself when it suffers rupture, a complication with a high mortality rate (> 80%). Its diagnosis is often incidental, usually during a radiological investigation related to other pathologies. Treatment consists of surgical correction that, when done electively, effectively prevents rupture and death.1 Thus, when this aneurysm is detected before rupture, presenting dimensions that justify elective precocious surgical correction (≥ 5.5cm), mortality is significantly reduced, making the benefit of early detection through screening to be considered. Based on epidemiological studies carried out in developed countries, it is estimated that the prevalence of AAA is 4-9% in men and 1% in women.2 Age significantly impacts the incidence of AAA. In fact, its incidence rises sharply in individuals over 65 years of age.3 In Portugal, there are only two studies on the prevalence of AAA. The first, provided by the screening program “Aorta não avisa”, developed by the Portuguese Society of Angiology and Vascular Surgery, estimated a prevalence of 2.2% for men over 60 years of age and 3.94% for men over the age of 65 years.4,5 The main risk factors for the development of this aneurysm are male gender, age ≥ 65 years, smoking at least 100 cigarettes throughout life, family history in 1st degree of AAA, the existence of other arterial aneurysms, arterial hypertension, and dyslipidemia.2
Based on this information, several international guidelines recommend screening AAA in men aged ≥ 65 years, especially those who have smoked at least 100 cigarettes in their lifetime.1,6
The purpose of this report is to present a case of AAA of generous dimensions, in a risky and apparently asymptomatic individual, diagnosed incidentally, as well as to reflect on the importance of implementing a screening program of AAA in men aged ≥ 65 years in Portugal, in terms of health benefits, which would consist of performing an abdominal ultrasound only once in a lifetime since this screening method is cost-effective, sensitive, specific, safe, acceptable, accessible to all target population and allows early therapeutic intervention.1,6-8
Case report
Seventy-five-year-old man, autonomous in daily life activities and living with his wife. As a medical history, we highlight the fact that he is a former smoker (80 pack-year) and has hypertension, dyslipidemia, type two diabetes mellitus, chronic obstructive pulmonary disease, and benign prostatic hypertrophy (BPH). The patient was medicated with losartan + hydrochlorothiazide 100/25mg daily, lercanidipine 10mg daily, bisoprolol 5mg daily, simvastatin 20mg daily, indacaterol + glycopyrronium 85/43 micrograms daily, and dutastreride + tamsulosin 0.5/0.4mg daily, with good control of the above-mentioned pathologies. Regarding the surgical history, the patient underwent transurethral resection of the prostate (TURP) in 2018, with complete resolution of the low urinary symptoms related to BPH. There were no known cases of AAA in other family members.
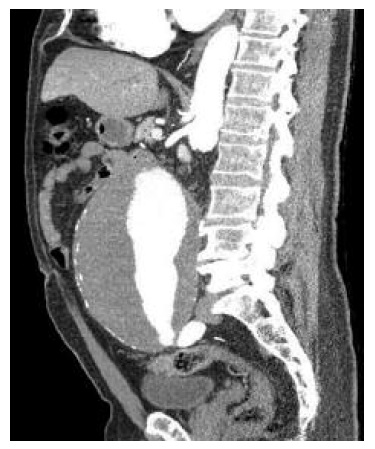
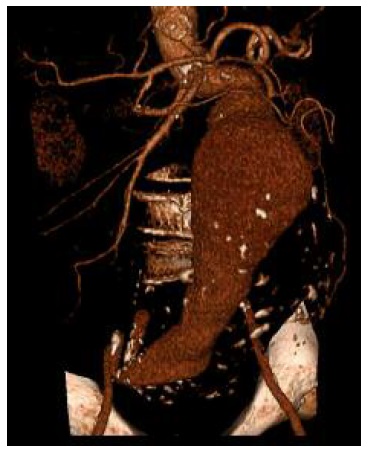
In September 2019, the patient was observed on a scheduled appointment with his family doctor, with a recurrence of low urinary complaints (nocturia and polaquiuria) for three months, with no other symptoms reported. In this consultation, an objective abdominal examination and urine test strip were performed, which showed no changes. Also, no signs of volume overload were identified, like oedema, hypertension, or pulmonary auscultation abnormalities. The urine culture and sediment were both normal. Suprapubic vesicoprostatic ultrasound was performed by a radiologist about three weeks later. During this examination, a moderately enlarged prostate (about 34cc) was observed, and it was incidentally detected, superior to the bladder, a massive AAA about 16cm long, 11cm anteroposterior caliber, and 6cm lumen patent, and in close contact with it. In view of these findings, the patient received from the radiologist the indication of the imperative need to go to the emergency department (ED). On the same day, the patient presented to the ED, where he underwent angiography by computed tomography (angio-CT) and tridimensional angio-CT (Figures 1 and 2). The patient was hospitalized and, after two days, the AAA was surgically corrected without complications. He was discharged at the end of the sixth postoperative day, with complete resolution of the urinary symptoms.
Comment
The present case illustrates the incidental detection of an AAA whose dimensions justified elective surgical correction (≥ 5.5cm).1,6 Bearing in mind that the patient's low urinary symptoms resolved after surgery, a AAA contribution to them cannot be excluded, through bladder compression by the aneurysm. Although AAA is rarely symptomatic before its rupture, when it is, low urinary symptoms are a frequent clinical manifestation, albeit very non-specific. According to Lazarus et al,9 71% of patients with AAA may have imaging evidence of ureteral obstruction caused by the aneurysm and, thus, high urinary symptoms. However, as mentioned, the patient in the present case had complaints of low urinary symptoms, which are less frequent in the context of AAA than high urinary symptoms. Regarding the present case, we are not able to establish a secure relationship between these symptoms and the AAA, at least exclusively since the patient had an enlarged prostate which can also contribute to them. However, the close contact between the AAA and the superior bladder makes a compression effect possible aggravating the symptoms caused by an enlarged prostate. Despite these considerations, the presence of low urinary symptoms in patients with BPH with optimized therapy and/or with no apparent cause should raise the suspicion of AAA, especially in men aged ≥ 65 years. The previous ultrasound did not confirm the existence of AA. The ultrasound performed before the TURP did not show the existence of an AAA. This could be explained since ultrasound is an operator-dependent examination as is the technique used. Probably, the progressive growth in the extension of the AAA explains why the first ultrasound failed to detect it, at that time. The guideline of the European Society of Vascular Surgery1 refers that the incidental diagnosis of AAA is frequent through imaging tests requested for the etiological study of symptoms such as chest pain, low back pain, abdominal pain, and low urinary symptoms, as was the case here. This case was taken to the Emergency Department because of the high risk of rupture and death, taking into account that AAA with > 7cm in diameter has a probability of rupture at one year of 33%.10 This case raises the question of the usefulness of an ultrasound populational screening program in Portugal for men aged ≥ 65 years, a population in which the present case is included and in which this aneurysm is more common. In addition, the high smoking burden significantly increases the risk of developing AAA, which inserts the case described in the group of individuals at higher risk for AAA and who would benefit most from screening. Based on several large-scale randomized clinical trials11-13 and meta-analyzes,14-16 there is strong evidence that this screening program in this population (men aged ≥ 65 years) would be cost-effective and significantly decreased the AAA-related mortality in other countries. This screening program is already implemented in the United Kingdom17 and in Sweden,18 where it has remained cost-effective and show to be effective in terms of secondary prevention. Besides that, the European Society of Vascular Surgery and the Canadian Task Force on Preventive Health Care guidelines1,6 recommend single screening for AAA by abdominal ultrasound in men aged ≥ 65 years. Bearing in mind that the prevalence of AAA in Portugal is similar to that estimated in the aforementioned studies (2.2-3.9%),4-5 it is plausible that the implementation of a screening program in this country will be clinically relevant, preventing AAA from growing to dimensions with a high probability of rupture and consequent risk of death, aiming the early detection of asymptomatic AAA and reduction of complications such as rupture and death.
In conclusion, given the higher incidence of AAA in men ≥ 65 years of age, ultrasound screening performed once in a lifetime in this population, which is safe and cost-effective, may contribute to lowering the mortality and morbidity related to this pathology.

