











 (pdf)
(pdf)




 SciELO
SciELO  SciELO
SciELO 
 Permalink
Permalink
Primary health care is the cornerstone of health care systems.1 Worldwide, 90% of all health-related contacts take place in primary care, but these encounters are only sparsely coded and therefore almost unavailable for research and policy purposes. As recognised by the World Organization of Family Doctors (WONCA), primary care needs to move forward by capturing core values through coding the content of the primary care domains. 2 The ICPC-33 offers the opportunity to solve this information gap in primary health care. The Brazilian Society of Family and Community Medicine (SBMFC) together with other members of the ICPC-3 Consortium and the WONCA International Classification Committee (WICC) contributed to the development of ICPC-3. 4
The classifications that are used today, in particular, the International Classification of Diseases (ICD) 5 and ICPC-16 and 27 are not built to capture person-center-edness, such as functions, activities, participation, and the personal environment, in one classification. 8 The emphasis of ICD is too much on hospital-related diseases and disorders, which requires a different classification. Self-limiting diseases and health problems as presented in primary health care practice, e.g., shoulder syndrome, neck syndrome and back syndrome are lacking in ICD.
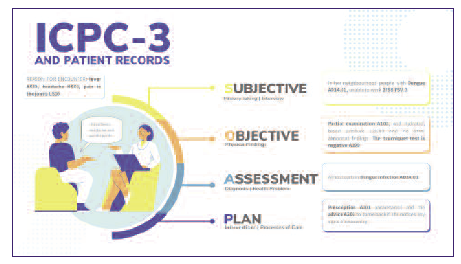
ICPC-3 has a few important improvements over ICPC-1 and ICPC-2. The list of (symptom) diagnoses has been updated to the latest insights and it has been made possible to consider regional differences in the coding of diseases and disorders. There is also (much) more space to register preventive activities (such as vaccinations) and care within integrated care programmes. All codes are linked to the codes of other important registration systems such as ICD-10, ICD-11, ICF, ICHI, and Snomed CT, which promotes uniform registration and interoperability, especially to specialist and hospital care. And, above all, ICPC-3 makes it possible to register not only medical diagnoses and interventions, but also many aspects of physical, psychological, and social (environmental) functioning. This also helps to focus on the essential problems of the patient when recording the consultation and not just on his medical diagnoses. Figure 1 is an example of a consultation coded with the ICPC-3.
The ICPC-3 is therefore in line with current and future developments in general practitioner care.

