











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Chronic spontaneous urticaria (CSU) is a heterogeneous disease characterized by the development of pruritic wheals and/or angioedema without relation to specific triggers, lasting longer than 6 weeks. When urticaria is uncontrolled despite optimal treatment, and/or systemic inflammatory symptoms appear, the presence of autoinflammatory syndromes should be investigated 1.
Schnitzler Syndrome (SchS) is a rare acquired autoinflammatory syndrome. An urticarial rash is present in all patients mostly affecting the trunk and limbs, consisting of slightly pruritic papules and plaques, lasting less than 24 hours that can be exacerbated by stress and physical exercise. Fever, arthralgia, bone pain, lymphadenopathy, and hepatosplenomegaly are also commonly present 2. Although monoclonal gammopathy is an obligate diagnosis criteria, eight cases have been reported of patients with clinical symptoms compatible with SchS without monoclonal gammopathy 3-9. Treatment is usually based on IL-1 blocking agents such as anakinra and canakinumab2.
We report the case of a 43-year-old female with CSU unresponsive to omalizumab that later developed systemic inflammatory symptoms. Two years prior she was diagnosed with chronic spontaneous urticaria with associated angioedema. She was medicated with antihistamines in a dose of four times per day, recurrent cycles of oral corticosteroids (at least 1/ month), and maintaining symptoms. She was then referred to a specialized urticarial center (Urticaria Center of Reference and Excellence - UCARE). At the first appointment, the patient reported outcome measures (PROM) were: weekly urticaria activity score (UAS7)=26, Urticaria control test (UCT)=2, and Dermatology Life Quality Index (DLQI)=21. During investigational workup autoimmune thyroiditis was diagnosed, with normal thyroid function. Total IgE was elevated (378 U/mL). The remaining investigation was unremarkable. Skin prick tests and autologous serum skin tests were not performed due to the inability to suspend antihistamines. The clinical diagnosis of uncontrolled CSU associated with delayed pressure urticaria was made and the patient was proposed to start omalizumab treatment. Omalizumab was started at a dosage of 300mg every 4 weeks (Q4W). After 3 months, the dosage was progressively increased to a maximum of 600mg Q4W, during more 3 months, with partial response.
She then began developing self-limited fever periods (37.5-38.5ºC) and arthralgias associated with edema and morning stiffness, involving finger, wrist, and knee joints. These symptoms occurred predominantly in the evening. Magnetic resonance imaging confirmed inflammatory changes in the wrist and knee joints. She self-medicated with non-steroidal anti-inflammatory and oral systemic corticosteroids (prednisolone 20mg/day), with transient improvement but without complete remission. Whenever corticosteroids were suspended, symptoms reappeared. An underlying autoinflammatory syndrome was suspected, prompting a clinical and laboratory reassessment.
The physical exam was unremarkable. Laboratory investigations were significant for microcytic anemia (Hb 11.1g/dL, VGM 76.2, HGM 25.5pg), elevated inflammatory parameters: CRP 3.09 mg/dL, erythrocyte sedimentation rate (ESR) 66 mm/h, ferritin 321 ng/mL, sérum amyloid A 362mg/L (RV:<6.4 mg/L). Complement levels, liver and renal functions were in normal ranges. Anti-nuclear antibody (ANA), anti-double strand DNA antibodies (anti-dsDNA), anti-neutrophil cytoplasmic antibody (ANCA), rheumatoid factor (RF), and cryoglobulin were negative. Free serum light chains were within reference value ranges and were undetectable in urine. Serum and urine immunoelectrophoresis showed no evidence of monoclonal gammopathy. The genetic sequencing of the NLRP3 gene showed no detectable mutations (Sanger sequencing). Histopathological analysis of the cutaneous lesions showed the presence of numerous neutrophils in the dermal papillae and ruled out vasculitis. Abdominal ultrasound showed no evidence of hepatomegaly or splenomegaly.
The patient presented with systemic inflammatory symptoms and signs and was unresponsive to treatment with omalizumab, leading to a presumptive diagnosis of autoinflammatory disease. She suspended omalizumab after 6 administrations of 600mg Q4W and started treatment with IL-1 receptor antagonist, anakinra (Kineret®, Swedish Orphan Biovitrum, Stockholm, Sweden) - 100 mg, subcutaneously injected daily. Cutaneous symptoms and fever resolved 24 hours after the first injection and musculoskeletal complaints resolved within 7 days. After 1 month of follow-up, the PROM were UAS7=0, UCT=16, and DLQI=0 (Figure 1).

Figure 1 Spontaneous and after skin scratching - red, swollen, itchy hives (wheals) and/or angioedema, with less than 24h individual duration, migratory, with no residual hyperpigmentation
After 3 months laboratory tests normalized (except for, a slight increase of serum amyloid A), without the development of monoclonal gammopathy or remarkable changes in IgM concentrations. Autoimmune thyroiditis remained controlled under treatment. Relevant testing trends in time are summarized in Table 1. After 12 months of follow-up, the patient remained asymptomatic.
Table 1 Laboratory investigation and urticaria activity evolution
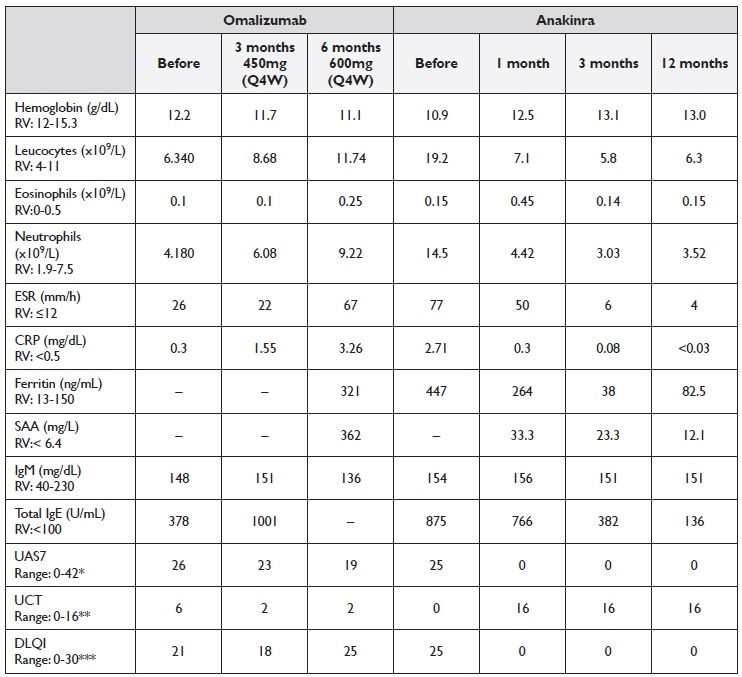
Q4W - every 4 weeks; ESR: Erythrocyte sedimentation rate; CRP - C-reactive protein; SAA - serum amyloid A; RV - Reference Value; UAS7 - weekly urticaria activity score; UCT - urticaria control test; Dermatology Life Quality Index - DLQI
* Controlled Urticaria defined by value ≤6; ** Controlled Urticaria defined by value ≥12; *** 0-1: does not affect quality of life, 2-5: mild impairment in quality of life, 5-10: moderate impairment in quality of life, 11-20: severe impairment in quality of life, 21-30: extreme impairment in quality of life
Given the age of onset, compatible symptoms, elevated inflammatory parameters, and complete and fast response with anakinra, we proposed the diagnosis of SchS, despite the absence of monoclonal gammopathy.
The role of IgM or IgG paraprotein in the pathogenesis of SchS remains unclear. It is not known if it precedes or follows the first clinical signs. In two of the cases in which monoclonal gammopathy was absent at presentation, patients developed IgM monoclonal gammopathy later during follow-up suggesting that cutaneous symptoms may precede typical laboratory findings 6,8.
Authors such as Husak et al. suggest that the SchS spectrum should be broadened, as monoclonal gammopathy can develop later on or never develop at all in patients with clinical characteristics otherwise compatible with the disease 7.
Very high clinical suspicion and an extensive workup to exclude alternative diagnoses are essential to diagnose SchS without monoclonal gammopathy. In our case lesions are uncharacteristic of urticarial vasculitis and the biopsy showed no evidence of vasculitis. Neutrophilicrich infiltrates are compatible with the lesions usually seen in patients with SchS. The absence of autoantibodies, cryoglobulins, and normal complemente excluded systemic lupus erythematosus and cryoglobulinemia2. Adult-onset Still’s disease (AOSD) is na inflammatory disorder characterized by spiking fever (>39ºC), cutaneous eruption, arthralgia, or arthritis.
The typical cutaneous eruption is rarely pruritic, have a salmon-pink color, appear predominantly in extremities, and comes and goes with daily fevers. Other symptoms frequently present in AOSD were absent in our patient such as lymphadenopathies, hepatomegaly, splenomegaly, sore throat, or abnormal liver enzymes 2.
Cryopyrin-associated periodic syndromes (CAPS) usually manifest in a younger age, have a positive family history, and are associated with mutations in gene NLRP3 2,9.
In CSU cases refractory to standard treatment, especially the omalizumab treatment and particularly when systemic inflammatory signs and symptoms develop, autoinflammatory diseases must be considered. Anti- IL-1 agents such as anakinra, canakinumab and rilonacept have been used successfully to treat patients with SchS. Initially, these drugs were used due to the clinical similarities with CAPS, however recent studies show an increase in IL-1β in patients with SchS 10.
Despite the absence of monoclonal gammopathy Schnitzler Syndrome should be considered, and treatment with IL-1 blocking agents initiated, to achieve complete symptom control and return quality of life to patients. Nevertheless, this remains a presumptive diagnosis as the patient fails to meet the criteria for the disease, we emphasize the need to perform an exhaustive differential diagnosis to exclude other causes. Broadening the spectrum of SchS would allow patients to be promptly treated with adequate drugs. Being a rare disease, prospective multicentric studies are needed to characterize patients who don’t fulfill the criteria yet drastically improve with anti-IL-1 drugs.

