English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Ventriculitis is the main complication of central nervous system (CNS) infection and is associated with high morbidity and mortality.1 This may be due to a brain abscess, primary bacterial meningitis, catheter-associated ventricular infection, neurosurgical site infection or bacteremia.2However, ventriculitis without concurrent CNS infection is rare.1,2
The authors present a case of a 55-year-old woman admitted to the emergency department for acute altered mental status, Glasgow coma scale 9. At admission she had high fever (40.1°C), confusion and altered mental status, without any neck stiffness nor other symptom of meningism.
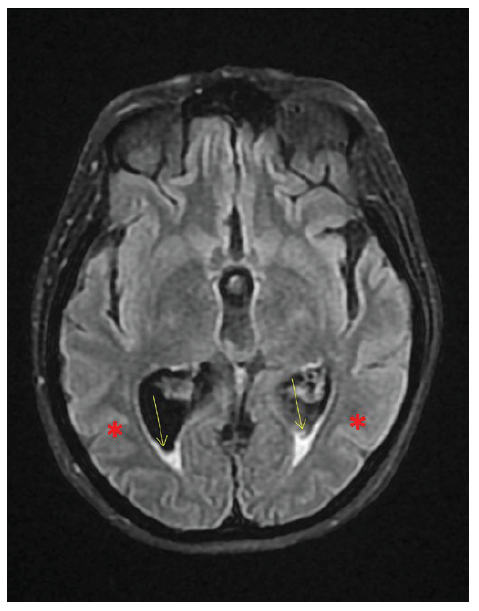
A computed tomography (CT) scan showed periventricular vasogenic edema but no lesion or another abnormality. Brain magnetic resonance imaging (MRI) showed massive intraventricular purulent collection deposited in the dependent parts of the lateral ventricles, third ventricle and IV ventricle as well as in cisterna magna, interpeduncular cistern, and in the lateral sulcus. Spinal tap revealed cloudy cerebrospinal fluid (CSF) with 7200/mm3 leukocytes, 95% polymorphonuclear, 5% mononuclear, glucose 1 mg/dL and total proteins 8528 mg/dL. Streptococcus pneumoniae was identified in CSF, and prompt antibiotic therapy with ceftriaxone was initiated, with improvement.
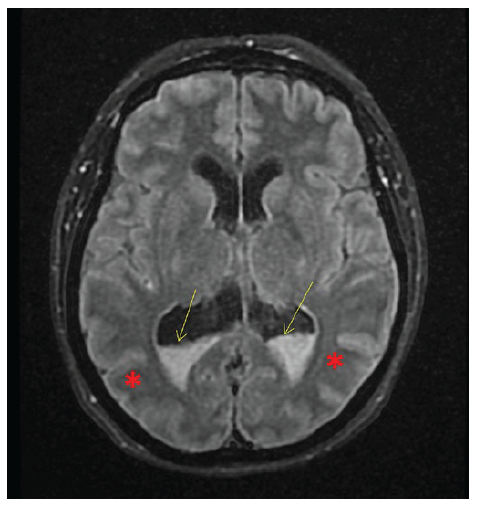
Figure 1 Brain MRI: massive intraventricular purulent collection deposited in the dependent parts of the lateral ventricles (yellow arrow), and oedema (*).