











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Ten-day-old female referred to a pediatric urology consultation due to prenatal diagnosis of left renal agenesis and a pelvic cystic image, which raised the suspicion of a nephro-urologic malformation.
At birth, analytically with normal values of Urea (34 mg/dl) and Creatinine (1.38 mg/dl). Ultrasound in the first week of life confirmed a hydrohematocolpos, showing a pelvic, non-pure, cystic image (Fig. 1), identified two hemi-uterus suggesting a didelphys uterus and a tubular image with bladder insertion adjacent to the left uterus, interpreted as a ureteral remnant.
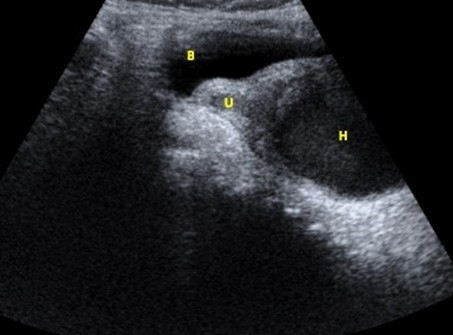
Figure 1: Pelvic ultrasound (longitudinal) showing the blader (B), the left hemi-uterus (U) and a hematocolpos of heterogenous content in the obstructed hemi-vagina (H).
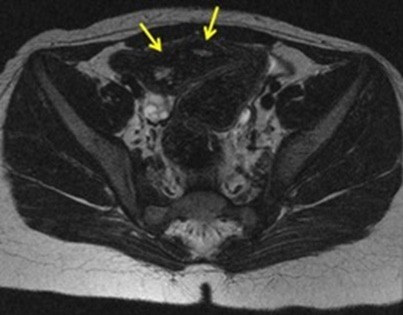
Hydrohematocolpos was drained to prevent infection. Magnetic resonance imaging was performed at 7 months of age, confirming left renal agenesis, a left ureteral remnant with ureterocele (Fig. 2) and a didelphys uterus (Fig. 3).
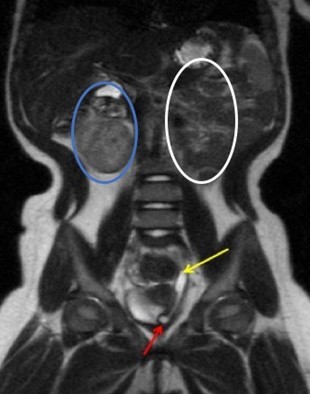
Figure 2: Coronal T2-weighted image demonstrating the presence of a right kidney (blue circle), absence of the left kidney (white circle), a left ureteral remnant (yellow arrow) and an ureterocele (red arrow).
Currently at 2 years-old, she remains asymptomatic and maintaining regular follow-ups with urologic pediatricians. OHVIRA (Obstructed hemivagina and ipsilateral renal anomaly) syndrome, also known by Herlyn-Werner- Wunderlich syndrome, is a congenital anomaly of the female urogenital tract resulting from an anomaly of the Mullerian and mesonephric ducts. It is characterized by a didelphys uterus with an obstructed/blind hemi-vagina and ipsilateral renal agenesis1 accounting for 0.16-10% of Mullerian duct malformations (MDM).
Patients are usually asymptomatic until puberty, when they begin to have dysmenorrhea and cyclic pelvic pain due to hematometrocolpos, as a consequence of obstructed hemi- vagina. In the postnatal period and early infancy, the same symptoms may occur due to the influence of maternal hormones.
Acute complications include pyohematocolpos and pyosalpinx, and long-term complications include endometriosis, pelvic inflammatory disease, and infertility.1 Differential diagnosis includes others MDM (bicornuate uterus, septate uterus), imperforate hymen and transverse vaginal septum.
Treatment is symptomatic, with vaginal septotomy for hematocolpos drainage. Hemi-hysterectomy is not indicated.2,3
As there is a strong association of female genital tract and renal anomalies, when the patient presents with one of these, a screening for associated anomalies should be performed.

