



![Seasonal Variability of [18F]FDG uptake in Brown Fat on the same Patient](/img/en/prev.gif)







 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Case Presentation
A 44-year-old man presented to the emergency department complaining of left scrotal pain, 5 days after falling from his own height in a sitting position. The patient referred a gradual worsening of the pain, without fever or other symptoms.
Physical examination revealed a little enlargement and tenderness in the left hemiscrotum, with a painful lump in the inferior portion of the testicle, which did not change after Valsalva maneuver.
Laboratory analysis signaled no relevant inflammatory markers.
A scrotal Doppler Ultrasound exam was performed, and when the probe was placed directly over the point of maximal tenderness, as indicated by the patient, it immediately revealed a dilated, noncompressible pampiniform plexus’ vein with echogenic intraluminal filling defect, and absent flow at color Doppler (Figure 1).
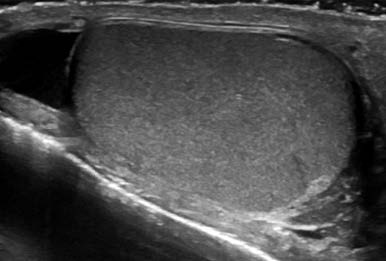
Mild hydrocele was also documented (Figure 2)
Both testicles and epididymis were symmetrical and had normal echotexture.
The patient underwent analgesic and anticoagulation treatment (enoxaparin - low molecular weight heparin) for 2 weeks, with bed rest, with good clinical results.
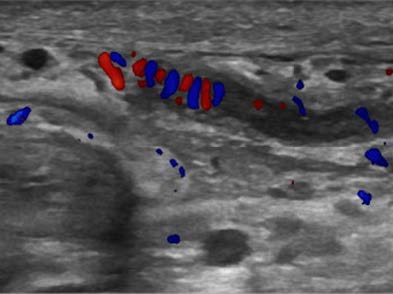
Figure 1: Left spermatic cord with a dilated, noncompressible pampiniform plexus’ vein with echogenic intraluminal filling defect (arrow).
Discussion
Spontaneous thrombosis of the pampiniform plexus is an uncommon entity responsible for painful scrotum. Left side thrombosis is most common. Anatomical particularities seem to justify left side preponderance.1
Pampiniform plexus thrombosis is being associated with coagulation abnormalities, retroperitoneal tumors, vigorous exercise, or anatomical factors, such as compression of the left renal vein by superior mesenteric artery (nutcracker syndrome), absent or incompetent valves of the testicular vein, or absence of inferior vena cava.2,3Although trauma is included in several articles as a cause of pampiniform plexus thrombosis, the authors did not find any similar case report.
Doppler ultrasound shows a tubular noncompressible structure, with more or less echogenic content, depending on temporal evolution, with no blood flow.
With spontaneous thrombosis of the pampiniform plexus, some differential diagnoses should be ruled out, and the most important is a retroperitoneal tumor. In this case, the authors assumed a traumatic cause for pampiniform plexus thrombosis, and management consisted of anticoagulation, painkillers and bed rest, and clinical follow-up. In fact, there are no formal guidelines to treat this entity,1 although a conservative approach, with anticoagulant and anti- inflammatory medication being considered the better management.1,3

