










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
Print version ISSN 2341-4545
GE Port J Gastroenterol vol.25 no.1 Lisboa Feb. 2018
https://doi.org/10.1159/000477763
IMAGES IN GASTROENTEROLOGY AND HEPATOLOGY
An Unexpected Abdominal Radiographic Finding: Chilaiditi Sign
Um achado radiográfico abdominal inesperado: Sinal de Chilaiditi
Rui Moraisa, Pedro Lopesb, Guilherme Macedoa
aGastroenterology Department and bInternal Medicine Department, Centro Hospitalar de São João, Porto, Portugal
* Corresponding author.
Keywords: Chilaiditi sign, Chilaiditi syndrome, Computed tomography
Palavras-Chave: Sinal de Chilaiditi, Síndrome de Chilaiditi, Tomografia computorizada
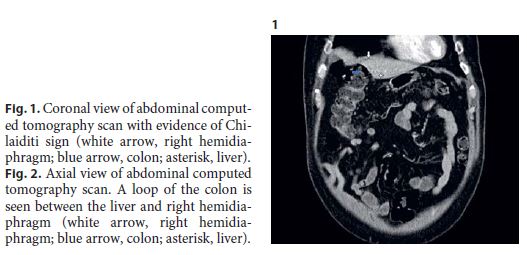
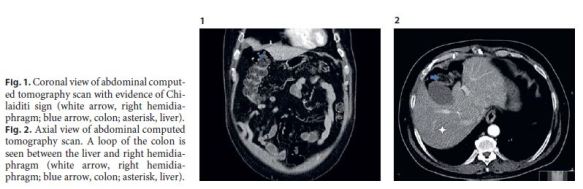
A 60-year-old male with a history of type 2 diabetes mellitus, diabetic nephropathy, and arterial hypertension, under isophane insulin and olmesartan treatment, presented to the emergency department due to profuse watery diarrhea (5–10 stools per day) for 2 weeks. He denied abdominal pain or other associated symptoms. Laboratory assessment revealed acute-on-chronic kidney disease and mild elevation of inflammatory biomarkers. An abdominal ultrasound and an abdominal X-ray were performed and were unremarkable. He was admitted to an intermediate care unit, and after aggressive intravenous hydration and antibiotherapy, he started to show clinical and renal function improvement. Stool cultures were negative. Nevertheless, 5 days after admission, he complained of epigastric pain, which was moderate, cramping, and nonradiating. The patient maintained 2 loose stools per day but denied nausea, vomiting, or other relevant symptoms. On physical examination, he presented slight epigastric tenderness. Laboratory testing was unremarkable. An abdominal computed tomography revealed a loop of colon between the liver and right hemidiaphragm, consistent with Chilaiditi sign (Fig. 1, 2).
This radiographic finding was initially described by the Greek radiologist Demetrius Chilaiditi in 1910. This condition has an incidence of 0.25–0.28% worldwide, being more frequent in men and the elderly [1] . The etiology can be congenital or acquired. It is usually incidental and asymptomatic; however, when it is associated with gastrointestinal symptoms, such as abdominal pain, constipation, or nausea, it is called Chilaiditi syndrome. Complications of Chilaiditi syndrome include volvulus of the cecum, splenic flexure or transverse colon, cecal perforation, and perforated appendicitis [2]. Chilaiditi syndrome is initially managed conservatively with rest, fluid therapy, and laxatives. Surgical intervention is only indicated when severe complication occurs [1]. In our patient, since other causes of epigastric pain, such as pan creatitis, cholangitis, or acute myocardial infarction, were excluded and admission abdominal X-ray was normal, we can conclude that this symptom was most likely related to Chilaiditi sign. A possible pathophysiologic explanation might be stretching of the right hemidiaphragm due to colonic interposition leading to epigastric pain. Due to the patients comorbidities, we took a conservative approach with fluid therapy, rest, and close observation. Epigastric pain subsided completely after 24 h. There was no pain recurrence during hospital stay. The patient was observed 6 months later in the outpatient clinic and remained asymptomatic.
Chilaiditi sign and Chilaiditi syndrome are rare conditions that are often misdiagnosed in clinical practice. Since they can be associated with severe complications, it is important to recognize them on presentation in order to prevent unnecessary exams and surgical interventions.
References
1 Kang D, Pan AS, Lopez MA, Buicko JL, Lopez-Viego M: Acute abdominal pain secondary to Chilaiditi syndrome. Case Rep Surg 2013;2013:756590. [ Links ]
2 Moaven O, Hodin RA: Chilaiditi syndrome: a rare entity with important differential diagnoses. Gastroenterol Hepatol 2012;8:276–278. [ Links ]
Statement of Ethics
This study did not require informed consent nor review/approval by the appropriate ethics committee.
Disclosure Statement
There are no conflicts of interest to declare.
* Corresponding author.
Dr. Rui Morais
Gastroenterology Department, Centro Hospitalar de São João
Alameda Professor Hernâni Monteiro
PT–4200-319 Porto (Portugal)
E-Mail ruimorais20@gmail.com
Received: February 21, 2017; Accepted after revision: May 12, 2017

