










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
Print version ISSN 2341-4545
GE Port J Gastroenterol vol.26 no.4 Lisboa Aug. 2019
https://doi.org/10.1159/000492068
IMAGES IN GASTROENTEROLOGY AND HEPATOLOGY
Splenic Rupture following Transnasal Endoscopy
Rotura Esplénica após Endoscopia Transnasal
Mariana Ferreira Cardoso, Gonçalo Alexandrino, Rita Carvalho
Gastroenterology Department, Hospital Professor Doutor Fernando Fonseca, Amadora, Portugal
* Corresponding author.
Keywords: Splenic rupture, Transnasal endoscopy, Ultraslim gastroscope
Palavras-Chave: Rotura espénica, Endoscopia transnasal, Endoscópio ultra-fino
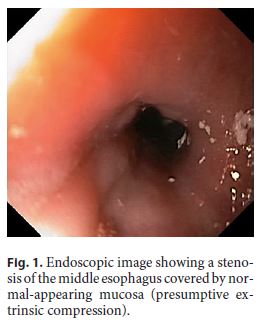
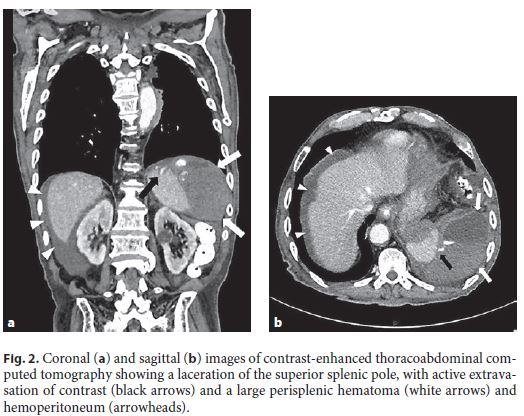
We present the case of an 82-year-old Caucasian male with a known medical history of ischemic heart disease and atrial fibrillation under anticoagulation with apixaban who was admitted with dysphagia for solids and liquids starting 1 month before. On physical examination, he was malnourished and dehydrated. Laboratory workup showed a hemoglobin level of 12 g/dL, INR 1.0, and aPTT 24 s. Upper endoscopy revealed a stenosis of the middle esophagus covered by normal-appearing mucosa (presumptive extrinsic compression), which could not be passed with the conventional gastroscope (outer diameter: 9.2 mm) (Fig. 1). After forceps biopsies of the stenosis, transnasal endoscopy was performed using the ultraslim gastroscope (outer diameter: 5.2 mm), which allowed passing the stenosis and placing a feeding tube. Immediately after the procedure, the patient complained of severe left abdominal pain and became hypotensive and tachycardic. His abdomen was tender with guarding over the left quadrants. His hemoglobin level initially dropped from 12 to 8 g/dL and reached a minimum of 6 g/dL, requiring transfusion of 2 packed red blood cell units. The patient was started on intravenous fluids, and anticoagulation (which had been switched to subcutaneous enoxaparin 2 days before) was withheld. After unremarkable chest and abdomen radiographs, contrastenhanced thoracoabdominal computed tomography showed a laceration of the superior splenic pole, with active extravasation of contrast and a large perisplenic hematoma and hemoperitoneum (Fig. 2a , b). It also revealed a 45-mm heterogeneous mass between the aorta, esophagus, and left main bronchus. The patient was managed conservatively and made an adequate recovery. After 2 weeks, he underwent endoscopic ultrasonography with fine-needle aspiration of the mediastinal mass, which was inconclusive. He later suffered a cardioembolic stroke and eventually died from a hospital-acquired pneumonia.
Splenic rupture is a rare but increasingly recognized complication of colonoscopy [1]. Its occurrence following upper endoscopy is even rarer, with very few cases reported in the literature [2–5]. It is thought to result from the excessive stretching of splenodiaphragmatic ligaments and splenoperitoneal lateral attachments during endoscopy [4, 5]. To the best of our knowledge, this is the first case attributable to the ultraslim gastroscope.
References
1 Barbeiro S, Atalaia-Martins C, Marcos P, Nobre J, Gonçalves C, Aniceto C: Splenic rupture as a complication of colonoscopy. GE Port J Gastroenterol 2017;24:188–192. [ Links ]
2 Hunter RC Jr: Gastroscopy and delayed rupture of the spleen; a review and report of a possible case. Gastroenterology 1955;29:898–906. [ Links ]
3 Lewis FW, Moloo N, Stiegmann GV, Goff JS: Splenic injury complicating therapeutic upper gastrointestinal endoscopy and ERCP. Gastrointest Endosc 1991;7:32–633.
4 Estevez-Boullosa P, Alonso-Aguirre PA, Couto-Worner I, Blanco-Rodriguez M, de Llano-Monelos P, Sanchez-Gonzalez F: Splenic rupture following a diagnostic upper endoscopy. World J Gastrointest Endosc 2010;2:35–236.
5 Jabr F, Skeik N: Spleen rupture complicating upper endoscopy. Endoscopy 2012;44:206–206. [ Links ]
Statement of Ethics
This study did not require informed consent or review/approval by the appropriate ethics committee.
Disclosure Statement
The authors have no conflicts of interest to disclose.
* Corresponding author.
Dr. Mariana Ferreira Cardoso
Gastroenterology Department
Hospital Professor Doutor Fernando Fonseca, IC-19 Venteira
PT–2720-276 Amadora (Portugal)
E-Mail marianafcardoso@gmail.com
Received: June 2, 2018; Accepted after revision: July 3, 2018
Acknowledgements
We would like to acknowledge the help provided by Dr. Maria Clara Aleluia (Imagiology Department) with radiologic imaging. We also thank Dr. David Horta, Dr. Alexandra Martins, Dr. Catarina Rodrigues (Gastroenterology Department), and Dr. Filipa Rocha (General Surgery Department), who were involved in the care of this patient.

