










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
Print version ISSN 2341-4545
GE Port J Gastroenterol vol.26 no.6 Lisboa Dec. 2019
https://doi.org/10.1159/000497386
ENDOSCOPIC SNAPSHOT
Deceptive Presentation of Infectious Esophagitis
Apresentação enganadora de esofagite infecciosa
Rui Mendoa, Catarina Félixa, Pedro C. Figueiredoa,b
aDepartment of Gastroenterology, Centro Hospitalar de Lisboa Ocidental, Hospital de Egas Moniz, Lisbon, Portugal; bDepartment of Gastroenterology, Hospital da Luz, Lisbon, Portugal
* Corresponding author.
Keywords: Infectious esophagitis, Herpes simplex, Candida esophagitis
Palavras-Chave: Esofagite infecciosa, Herpes simplex, Esofagite por Candida
A 23-year-old male without relevant medical history presented with a 3-day history of odynophagia, mixed dysphagia, and fever (maximum temperature 38,4ºC). Laboratory studies showed mild leukocytosis (12,000/ μL). An upper gastrointestinal endoscopy was performed and showed numerous scattered and coalescing, rounded, white plaques in the mid-esophagus (Fig. 1), circumferentially involving the distal esophagus (Fig. 2). Esophageal biopsies were obtained. After the endoscopy, the patient was started on acyclovir and fluconazol pending biopsy results. He tested negative for human immunodeficiency virus and was otherwise non-immunocompromised. Histologic examination showed eosinophilic inclusions (Cowdry type A inclusion bodies). Immunohistochemistry confirmed infection by herpes simplex virus. Fluconazol was therefore discontinued after 4 days of therapy, and acyclovir was continued with a total duration of 7 days. Symptoms resolved, allowing for hospital discharge after 5 days.
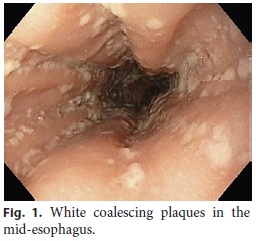
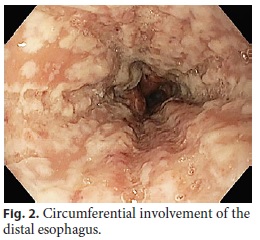
We present this unusual case of herpes esophagitis in a young immunocompetent patient due to the discordance between the clinical scenario suggesting viral infection and the endoscopy findings more typically found in Candida esophagitis.
Infectious esophagitis is the third leading cause of esophagitis after gastroesophageal reflux disease and eosinophilic esophagitis and it is more common in the immunocompromised host [1]. Candida organisms are the most common cause of esophageal infection [1]. Viral esophagitis is probably the second most common cause and it is typically characterized by odynophagia, retrosternal pain, and fever [2]. Typical endoscopic findings of herpes esophagitis include discrete or coalescent ulcerations of the mid-distal esophagus [1–3]. Nonetheless, it is important to remark that herpes esophagitis can be characterized by white plaques adherent to the esophageal mucosa, typically found in Candida esophagitis.
References
1 Hoversten P, Kamboj AK, Katzka DA. Infections of the esophagus: an update on risk factors, diagnosis, and management. Dis Esophagus. 2018 Dec;31(12):1–9. [ Links ]
2 Wilcox CM. Overview of infectious esophagitis. Gastroenterol Hepatol (N Y). 2013 Aug;9(8):517–9. [ Links ]
3 Kato S, Yamamoto R, Yoshimitsu S, Shimazaki K, Ogawa S, Itoh K, et al. Herpes simplex esophagitis in the immunocompetent host. Dis Esophagus. 2005;18(5):340–4. [ Links ]
Statement of Ethics
The authors declare that this case did not require informed consent or review/approval by the appropriate ethics committee.
Disclosure Statement
The authors declare that they have no conflicts of interest to disclose.
* Corresponding author.
Rui Mendo
Department of Gastroenterology, Centro Hospitalar de Lisboa Ocidental Hospital de Egas Moniz, Rua da Junqueira nº126
PT–1349-019 Lisbon (Portugal)
E-Mail mendorui@gmail.com
Received: December 13, 2018; Accepted after revision: January 27, 2019

