











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
Retrorectal cystic hamartoma, also called tailgut cyst (TGC) is an uncommon congenital developmental cystic lesion of the presacral area [1]. It arises from postnatal primitive tail gut remnants, which normally involute by the 8th week of development [2]. It is usually incidentally detected in middle-aged women, with a female-to-male ratio of 3:1 [3]. TGCs are asymptomatic in half of the patients; when symptomatic, they have the compressive effect of a growing mass in the pelvis. Due to the nonspecific nature of the symptoms and the complex anatomical location, a diagnosis is often challenging.
We report an uncommon case of rectal bleeding in an elderly male patient diagnosed as TGC, highlighting the importance of imaging in assessing the characteristics and extension before surgery.
Case Report
A 70-year-old male presented with hematochezia and perianal pain during defecation for 4 months. There was no history of abdominal pain, constipation, weight loss, or mass prolapsing through the rectum. Pallor was observed on general examination. Rectal examination revealed a palpable mass just above the dentate line. The hemoglobin level was 9 g/dL, and a peripheral smear demonstrated microcytic hypochromic anemia. Colonoscopy demonstrated a mucosal bulge in the posterior rectal wall (Fig. 1).
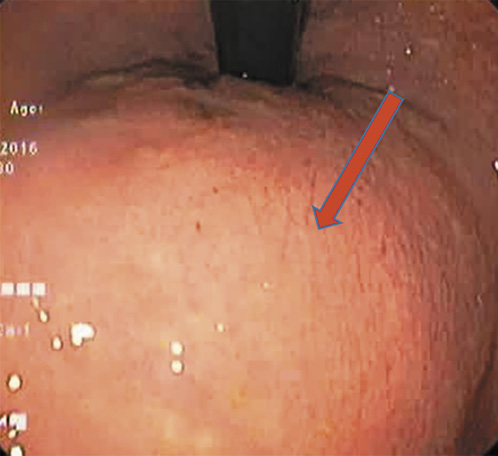
Fig. 1 Colonoscopy demonstrating a mucosal bulge in the posterior wall of the rectum (red solid arrow).
Abdominal and pelvic computed tomography (CT) showed a well-defined hypodense lesion 7.2 × 6.8 cm in size in the perianal space compressing the rectal and anal canal anteriorly. Pelvic magnetic resonance imaging (MRI) showed a 6.3 × 6.5 × 8.5 cm well-defined unilocular mass in the retrorectal compartment appearing hyperintense on T2W and hypointense on T1W images with mild peripheral enhancement (Fig. 2a, b). Anteriorly, it compressed the rectum without visible communication, and no invasion of adjacent structures was documented.
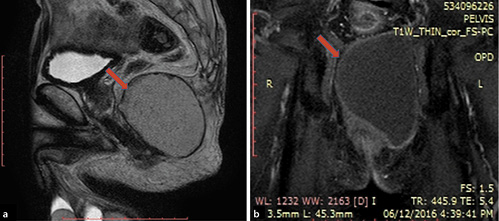
Fig. 2 a Pelvic MRI demonstrating a retrorectal mass displacing the rectum anteriorly and extending inferiorly beyond the coccyx. The mass shows hyperintensity on T2W imaging with mild peripheral enhancement (solid red arrow). b The retrorectal mass demonstrates hypointensity on T1W imaging (solid red arrow).
Radial endoscopic ultrasound (EUS) demonstrated a well-defined cystic lesion with some hyperechoic content surrounded by a distinct hypoechoic layer measuring 7.6 × 4.7 cm arising in the perirectal area above the anal verge (Fig. 3). No involvement of the rectal wall and sphincter complex was documented. Adenopathies were not identified.
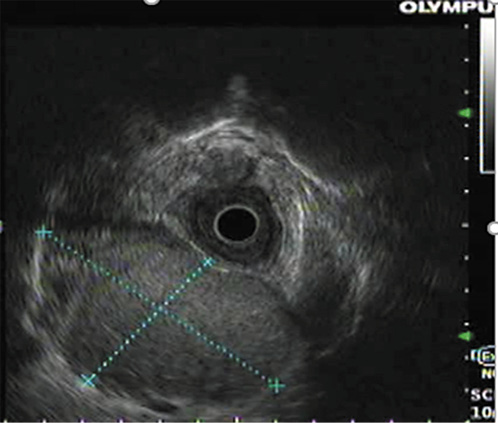
Fig. 3 Radial EUS demonstrating a well-defined cystic lesion 7.6 × 4.7 cm in size in the perirectal area, above the anal verge, with a distinct hypoechoic layer around it.
The patient was operated through a perianal approach, and complete excision of the cyst was achieved. Gross examination revealed an irregularly shaped ovoid multiloculated cyst measuring 7 × 5 cm in the greatest diameter (Fig. 4). On histopathology, the cyst wall lining consisted of a stratified squamous epithelium and mixed inflammation with foreign body giant cell reaction with thick fibrocollagenous tissue underneath (Fig. 5a, b). There was no evidence of malignancy or ectopic tissue. This confirmed the diagnosis of a TGC. The patient was discharged and is being followed in the outpatient department without recurrence.
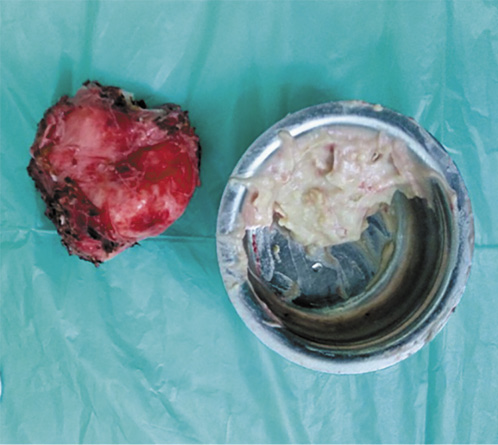
Fig. 4 The cyst was completely excised by a posterior approach. Grossly, the cyst measured 7 × 5 cm and was ovoid and multiloculated.
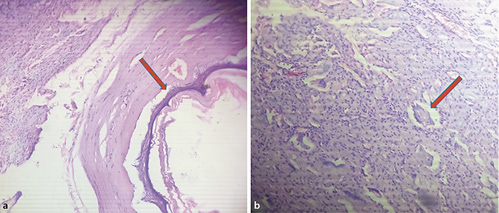
Fig. 5 a Cyst wall showing a stratified squamous epithelial lining with thick fibrocollagenous tissue underneath (red solid arrow). The subepithelium shows dense mixed inflammation. Hematoxylin-eosin. Original magnification, ×20. b Cyst wall lining showing mixed inflammation with numerous foreign body giant cells (red solid arrow). Hematoxylin-eosin. Original magnification, ×80.
Discussion
The retrorectal space is a loose areolar tissue plane consisting of totipotent cells, confined by the posterior rectal wall anteriorly and the sacrum posteriorly. The ureter, sacral nerve roots, and iliac vessels form the lateral border of this space [4]. Retrorectal lesions are rare clinical entities, with reports estimating an incidence of 1:40,000 to 63,000 [5]. These cysts are classified as teratomas or dermoid, neurenteric, epidermoid, or enteric cysts (TGCs and rectal duplication cysts) depending on the embryonic cells of origin [6]. They are more common among middle-aged women, which is possibly related to a more significant number of cases incidentally detected during gynecological examinations. Among men, malignant lesions are more common, due to delays in diagnosis [7]. In our case, a TGC presented in the rare form of rectal bleeding in a male of advanced age.
Hjermstad and Helwig [8] reported 53 cases of TGC, of which 51% presented with perianal pain and none presented with rectal bleeding. Other presenting features are compressive symptoms like chronic constipation, urinary retention, recurrent perianal infections causing retrorectal abscesses, or a history of multiple surgeries for anal fistulae [9]. The use of CT, MRI, and EUS has improved physicians’ ability to diagnose these rare tumors. Cystic, solid, or mixed lesions can be distinguished on pelvic CT or MRI delineating soft tissue planes and demonstrating the relationship of the lesions with the sacrum, muscles, and nerves. MRI has been shown to be superior to CT in providing a correct diagnosis of the type of retrorectal tumor, but the radiological diagnosis correlated with histopathology in only 16% to 28% of the cases for CT and MRI, respectively [10].
EUS fine-needle aspiration (FNA) of the cystic lesion is not advised, due to the low diagnostic yield and risks of cyst infection and of spilling malignant cells. However, there have been a few case reports indicating the utility of EUS FNA in the diagnosis of such lesions [11, 12]. The role of EUS FNA in these tumors requires further validation, and biopsy can be attempted only when the risk of malignancy by other imaging modalities has been excluded. Considering the above facts, EUS-guided FNA was not performed on our patient. In the present case, the imaging modalities narrowed down our hypothesis to a rectal duplication cyst and TGC. Its differentiation based only on these examinations is very challenging.
Our patient underwent a complete cyst excision by the posterior approach, and the intraoperative findings indicated no invasion of the rectal wall. Complete surgical resection and histopathology remain the mainstay of both diagnosis and definitive treatment. An anterior (transabdominal) approach is reserved for lesions above the sacral promontory and a posterior approach for lesions below the sacral promontory [13]. A combined approach may be used for large tumors extending on either side of the promontory [14]. Sakr et al. [15], in their single-center experience of 24 TGCs, performed excisions by an anterior (transabdominal), posterior (paracoccygeal), and combined (anterior plus posterior) approach for supralevator, infralevator, and multilocular cysts larger than 10 cm, respectively. To prevent recurrence and potential malignant transformation, complete excision is advised. Malignant transformation of the cyst into an adenocarcinoma, especially in males, confers a poor prognosis [13]. Nicoll et al. [16], in a recent systematic review, reported malignant transformation in 26% of their TGCs, with a male predominance. Sakr et al. [15] reported malignancy in 8% of their 24 cases of TGC.
The cyst was multiloculated on gross examination, and histopathology demonstrated that the cyst wall was lined by a stratified squamous epithelium with areas of inflammation and giant cell reaction and fibrocollagenous tissue. Hjermstad and Helwig [8] reported the majority of lesions as multiloculated and multicystic with a wide range of epithelial types lining the cyst wall. The most commonly encountered was squamous metaplasia, secondary to inflammation. A well-developed smooth muscle layer with a nerve plexus and a cyst lining by villi, crypts, and glands differentiate rectal duplication cysts from TGCs [17]. Teratomas and dermoid cysts differ from TGCs by the presence of components from the three germ layers.
A diagnosis of TGC was established in our patient considering the presacral location and multilocular nature of the cyst lined by squamous epithelial cells on histology. This report adds to the sparse literature on TGCs, in this case presenting in an advanced aged male with rectal bleeding. Different imaging modalities may show specific signs, but the core of diagnosis and treatment remains histopathology and surgical excision, respectively.

