











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
Although its incidence is declining worldwide, gastric cancer remains a frequent cause of cancer-related mortality. Indeed, this neoplasia is often diagnosed at an advanced stage, when the 5-year survival is <5% [1]. Moreover, the prevalence is expected to remain high in the next decade due to the increasing population ageing [2]. Screening programs were found to distinctly improve patients’ survival by anticipating a cancer diagnosis [3]. Nevertheless, screening is applicable only in areas with a high incidence of gastric cancer, such as Korea, Japan, and China [4]. In Caucasian populations, identification and follow-up of gastric precancerous lesions - atrophy and intestinal metaplasia (IM) - is the only practical procedure aimed at increasing the diagnosis of cancer at an early stage. Indeed, patients with extensive IM, i.e., diffused on both antrum and gastric body mucosa, have a distinctly high risk of developing neoplasia and deserve a scheduled follow-up according to the current guidelines [5]. This approach was recently suggested also for areas with a low incidence of gastric cancer, such as the USA, at least in population subgroups at an increased risk [6]. Is there an optimal age threshold for searching for extensive IM on gastric mucosa in Western countries with a low-intermediate gastric cancer incidence? We conducted the present study to answering this clinically relevant question.
Materials and Methods
This is a post hoc analysis of prospectively collected data. In detail, a nationwide study involving 24 endoscopy units enrolled consecutive Italian patients aged between 50 and 65 years between January 2012 and March 31, 2012 [7]. Patients were referred for upper endoscopy from general practitioners due to upper gastrointestinal symptoms. Those who had previously undergone gastroscopy were excluded. All patients underwent endoscopic examination with standard biopsy sampling to search for Helicobacter pylori infection and gastritis staging according to the updated Sydney System mapping. Briefly, 2 biopsies from the antrum, 1 from the angulus, and 2 from the gastric body were used for both histological and H. pylori infection assessments. For the purposes of this study, only the presence and distribution of IM on gastric mucosa were considered. From the original database, information on age, sex, BMI, smoking habits, a first-degree family history of gastric cancer, and the main symptom was acquired. Symptoms were categorized as dyspeptic, gastro-oesophageal reflux, or both.
Data were compared in a univariate analysis using the χ2 test, or the Fisher’s exact test, as appropriate. A logistic regression analysis was performed by using extensive IM in the stomach as the dependent variable and age, sex, smoking, first-degree family history of gastric cancer, BMI, and type of symptoms as independent variables. Age was categorized into the following subgroups: 50-54, 55-59, and 60-65 years. Patients were considered to have a normal weight when their BMI was in the range of 18.5-24.9. Statistical analyses were performed using MedCalc® Statistical Software version 19.5.1 (MedCalc Software Ltd., Ostend, Belgium; https://www.medcalc.org; 2020).
Results
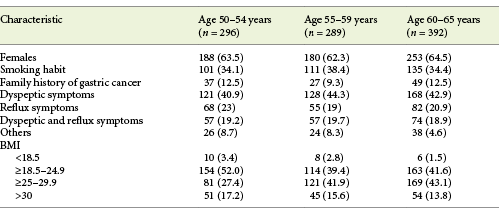
Data for 977 patients were available, including 456 (46.7%) males, 247 (25.3%) smokers, 431 (44.1%) with a normal BMI, and 113 (11.6%) with a first-degree family history of gastric cancer (Table 1). At the histological assessment, H. pylori infection was detected in 333 (34.1%) patients, extensive IM metaplasia was found in 35 (3.6%) patients, focal IM was found in 187 (19.1%) patients, and extensive atrophy without IM was found in 51 (5.2%) cases.
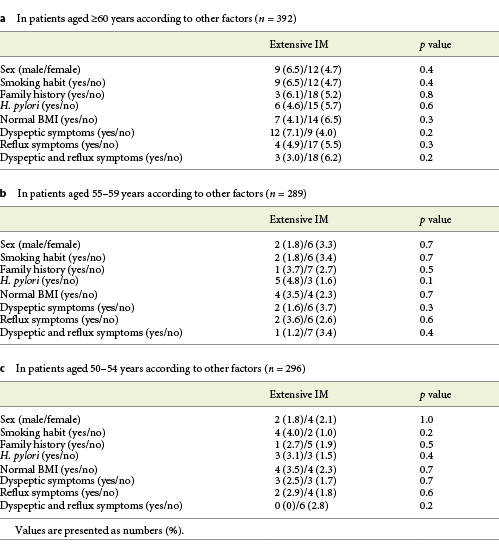
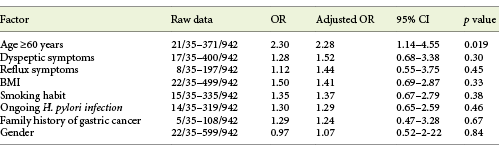
In the univariate analysis, the prevalence of extensive IM was 2% and 2.8% in patients aged 50-54 and between 55 and 59 years, respectively, and it increased to 5.4% in those aged 60-65 years, with a statistically significantly difference (p = 0.014) between patients aged 50-59 and those aged 60-65 years. In the latter patient group, although the values of extensive IM prevalence were higher in males and in patients with dyspeptic symptoms, as was the presence of a family history of gastric cancer, a smoking habit, or abnormal weight, the differences were not statistically significant (Table 2a). Similarly, no differences emerged in other age groups (Table 2b, c). In the multivariate analysis, only age >60 years was a factor independently associated with an increased prevalence of extensive IM (Table 3), with an adjusted OR of 2.28 (95% CI 1.14-4.55).
Discussion/Conclusion
Gastric cancer remains a neoplasia with a dismal prognosis when diagnosed at an advanced stage [1]. Unfortunately, screening programs successfully implemented in Asian populations are not practicable in areas with a low-intermediate incidence. Therefore, identification and scheduled follow-up of precancerous lesions on gastric mucosa is a plausible approach aimed at discovering noninvasive neoplasia or early gastric cancer, and the identification of high-risk groups would reduce the endoscopic surveillance burden and related costs [5]. Therefore, we investigated whether age and some clinical characteristics predict the presence of extensive IM in the stomach. Our data found that the prevalence of extensive IM was distinctly increased in patients aged 60-65 years, with a 2.28-fold increased risk compared to younger (age 50-59 years) subjects. None of the other considered factors emerged as an independent predictor in the multivariate analysis.
From the point of view of potential screening, we focused our investigation on extensive IM and in subjects aged 50-65 years based on some considerations. Among gastric precancerous lesions, the diagnosis of IM (k = 0.87) is distinctly more accurate than that of atrophy (k = 0.64) [8], and extensive IM harbors a gastric cancer risk that is twice that of extensive atrophy [9, 10]. Moreover, IM - but not atrophy - is accurately detected and staged at virtual chromoendoscopy, with an undoubted advantage for patient selection [11]. Therefore, extensive IM might represent an appropriate target for secondary prevention of gastric cancer [10]. On the other hand, subjects with an age ranging from 50 to 65 years could represent a potential target population for screening. Age ≥50 years is the lower threshold recommended by Italian guidelines for performance of an upper endoscopy in dyspeptic patients [12]. Moreover, we limited the evaluation to 65-year-old subjects because the gastric cancer incidence in Italy is 4-5 times higher in subjects aged >70 years [13]. These data were confirmed in a recent study showing that age >70 years was associated with a 9-fold higher probability of development of gastric epithelial neoplastic lesions in patients with gastric precancerous lesions [14]. It has been suggested that screening programs for gastric cancer in intermediate-risk European countries could be cost-effective if combined with a scheduled screening colonoscopy starting at 50 years of age [15]. Based on the data of present study, upper endoscopy could be proposed to 60- to 65-years-old subjects, allowing the identification of high-risk patients who require a scheduled follow-up.
In conclusion, upper endoscopy performed at age 60 years in dyspeptic patients allows optimization of the possibility of detecting extensive IM and identifying the small (5.4%) patients subgroup in need of a scheduled follow-up. Therefore, when deciding on occasional gastric cancer screening in Western populations, the choice of a cut-off age >60 years might be appropriate.

