











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Typhoid fever is a sporadic disease in developed countries and the majority of patients do not require hospitalization. Complications may occur in up to 15% of cases [1], with lower gastrointestinal bleeding (LGIB) being one of the most common and usually arising during the third week of illness [2, 3]. Since the advent of the current antibiotic era, the incidence of LGIB has been decreasing, and is mainly managed conservatively [2].
A 54-year-old man presented to the emergency department with a 1-day history of persistent fever and epigastric pain. He was a consumer of free-range eggs. Blood analysis revealed an elevation of the inflammatory parameters. Empiric antibiotherapy with piperacillin/tazobactam was initiated. Three days after admission, the patient developed high-volume hematochezia and hypovolemic shock. His hemoglobin levels fell from 10.3 to 5.7 g/dL and 3 units of red blood cell concentrate were administered within 24 h. Emergency upper endoscopy was unremarkable. Colonoscopy revealed multiple scattered fresh blood clots around the ileocecal valve. Computed tomography showed a nonspecific thickening of the terminal ileum with no evidence of active gastrointestinal bleeding (Fig. 1). Elective ileocolonoscopy identified multiple depressed ulcers with elevated borders and some elevated areas of edema and hyperemia on the terminal ileum (Fig. 2). Blood culture samples were positive for Salmonella typhi resistant to chloramphenicol, ampicillin, and trimethoprim-sulfamethoxazole, and sensitive to ceftriaxone. These findings allowed the authors to definitively diagnose an enteropathy secondary to S. typhi complicated with severe LGIB. Antibiotherapy was shifted to ceftriaxone, according to the antibiogram. There was a complete resolution of symptoms.

Fig. 1 Computed tomography. Thickening of the terminal ileum (white arrow) and cecum (yellow arrow).
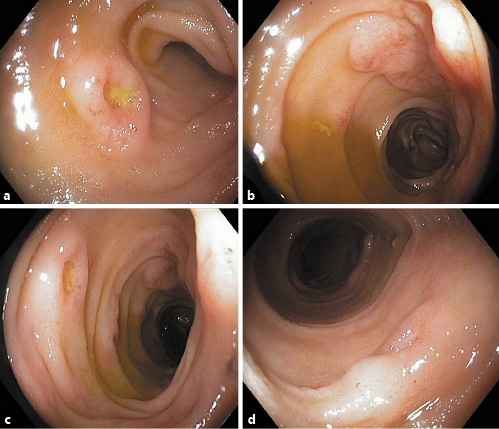
Fig. 2 Ileocolonoscopy. Terminal ileum: multiple depressed ulcers with elevated borders and some elevated areas of edema and hyperemia.
S. typhi is an enteroinvasive, Gram-negative bacteria that causes typhoid fever [4, 5]. The proliferation of this microorganism leads to the hyperplasia of lymphoid follicles of multiple organs, including the gastrointestinal tract [2, 3]. When reaching the submucosa, this hyperplasic tissue may ulcerate and erode vessel walls, causing bleeding [2]. The terminal ileum is particularly prone to the overgrowth of lymphoid tissue, being at a greater risk of hemorrhage [2, 3]. Except when severe and life-threatening, most LGIB cases do not require intervention and are managed conservatively [2]. In our report, no active bleeding was detected when the ulcers were observed, so endoscopic therapy was not performed.
Despite the scarcity of recent reports on typhoid fever complicated with significant LGIB, this case demonstrates it is still paramount to include this disease as a cause of severe LGIB. It further illustrates the importance of performing an early ileocolonoscopy, to be able to identify the bleeding location. We would also like to highlight the early onset of this hemorrhagic enteropathy, as it rarely occurs before the third week of disease progression [2, 3].

