











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkA 48-year-old male presented 3 days after laparoscopic cholecystectomy with recurrent right upper quadrant pain and laboratory cholestasis. The patient underwent endoscopic retrograde cholangiopancreatography (ERCP) after endoscopic ultrasound identifying distal choledocholithiasis and a small periampullary diverticulum (PAD). Conventional ERCP confirmed the presence of a PAD with a small opening unsuitable for duodenoscope entry with the distinct localization of the papilla obscured (Fig. 1a). Albeit a small bulge at 7 o’clock was noted, duodenoscope-guided eversion maneuvers were not attempted due to an awkward angle. Therefore, we switched to a cap-fitted, double-lumen upper endoscope and applied gentle suction at the lower PAD rim, resulting in prompt exposure of the papilla (Fig. 1b). Despite adequate stabilization in the cap (Fig. 1c), initial attempts of intra-cap cannulation failed, prompting us to re-switch to duodenoscope technology. After provisions had been made to potentially switch to a clip application strategy, the papilla indeed proved to continue protruding toward the duodenal lumen. Biliary wire-guided cannulation thus succeeded at the first attempt, confirming pre-papillary bile duct stones on cholangiography (Fig. 1e). Complete stone extraction was performed after papillotomy (Fig. 1f). The postinterventional course was uncomplicated.
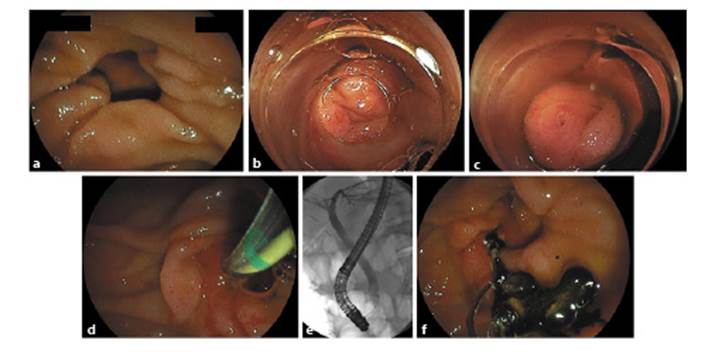
Fig. 1 a Duodenoscopic visualization of the small-necked periampullary diverticulum (PAD) without convincing identification of the papilla. b Cap-fitted, forward-viewing endoscopy after applying gentle suction over the lower rim of the diverticulum resulting in luminal eversion and exposure (post hoc the papilla most likely corresponds to the small mucosal bulge at 7 o’clock in a). c Stable positioning of the papilla into the cap with attempts to canulate the bile duct failing due to inadequate axis alignment. d Successful duodenoscope-guided biliary cannulation after re-switching scope technology with the papilla still exposed in the duodenum. e Confirmation of pre-papillary bile duct stone disease extracted by a Dormia basket after conventional papillotomy. f Successful stone extraction by a Dormia basket after papillotomy.
PAD may pose challenges in ERCP in terms of identification and exposure of the papilla as well as adequate axis alignment [1]. While forward-viewing endoscopic approaches with or without distal attachments have been described, suction eversion of a “hidden papilla” with subsequent duodenoscopy-guided ERCP has not yet been reported and may provide another trick of the trade in successful ERCP completion vis-à-vis PAD [2, 3].

