











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Background
Portuguese General Practice/Family Doctors (GP/FMD) have an increasing work-load with patients suffering from multimorbidity, defined as “any combination of chronic disease with at least one other disease (acute or chronic), biopsychosocial factor (associated or not) or somatic risk factor”,1 its prevalence being estimated as of 72.7% of adult patients, and particularly the elderly. (2 Portuguese population’s aging is a reality that increases the workload and responsibility for GP/FMD. (3
Multimorbidity is a common theme of research wi-thin GP/FMD. However, there are few studies primarily focused on the impact of the management of these complex patients on the quality of life and well-being of doctors, from a medical perspective. The first studies on this topic showed that doctors consider the management of these patients a complex diagnostic and therapeutic challenge, which often results in higher levels of distress among these healthcare professionals. (4
The validation of the ‘Questionnaire of Evaluation of Burden of Management of Multimorbidity in General Practice and Family Medicine’ (SoGeMM-MGF), a questionnaire that aims to evaluate how doctors perceive the burden of managing multimorbidity, was recently published in Portugal. It allows the evaluation of four impact areas of multimorbid patient management on doctors: negative feelings, cooperation, clinical work, and consultation workload. In the discussion chapter, the authors noticed the need to measure the psychological impact of the multimorbid patient’s management burden, considering other valid instruments, for SoGeMM-MGF only signals the problem. (5
Doctors’ well-being is a key player in providing high-quality healthcare. When at risk, it entails not only individual negative consequences but is also associated with lower therapeutic performance, translating into a higher rate of medical errors and reduced patient satisfaction with the care provided. (6-7
Anxiety and depression are two common psychological conditions among doctors. (8 In addition to individual factors, others such as work overload and difficult peer relationships have been identified as possible causal agents. (9 Even knowing that emotional dysfunction is related to high disability in the personal, social, and professional sphere of doctors, they often tend to neglect to feel unwell and rarely seek other specialist te-chnical help such as psychology or psychiatry. (10 This may impair their quality of life, which can and should be measured, (11 to implement strategies for its improvement.
In 2009, Kroenke and collaborators published the Patient Health Questionnaire for Depression and Anxiety (PHQ-4) scale, a screening tool for anxiety and depression that combines two subscales: Patient Health Questionnaire-2 (PHQ-2) and Generalized Anxiety Disorder-2 (GAD-2). (12 Comprising only four questions, which makes it highly practical, PHQ-4 was proven to be a valid and reliable screening tool for these pathologies, (13 having already been used in different studies. (14-15
PHQ-4 contains normative data which allows to assess the possibility of an individual suffering from anxious and depressive pathology. It is recommended to consider a total PHQ-4 sum to verify ‘yellow flags’ and ‘red flags’ and also to verify psychologic distress. (16
As doctors manage multimorbid patients, as older persons tend to have worse results and guidelines are ever more demanding and frequent, medical anxiety, depression, and distress can appear, and quality of life can worsen. After all, even differentiated doctors are persons.
Knowing that the PHQ-4 tool had not yet been adapted to the European spoken Portuguese this work’s objective was such accomplishment. Additionally, PHQ4’s concurrent validity with the psychological burden by the management of multimorbid patients (using the SoGeMM-MGF scale) and quality of life (using the European Quality of Life 5 Dimensions 3L scale, (EQ-5D-3L)) in a population of GP/FMD Portuguese specialists was intended.
Methods
The PHQ-4 scale was translated and cross-culturally adapted to European Portuguese following approval by the Health Ethics Commission of the Regional Health Administration (RHA) of Central Portugal (Administração Regional de Saúde do Centro). Permission has also been gathered from the original au-thor of all scales. This procedure entailed:
Translation: of the original scale from English to European Portuguese by two Portuguese experts. These experts were external to the study and had full professional working proficiency in English.
Linguistic verification: by three academic general practitioner experts, with previous experience in similar tasks and fluent in European Portuguese and English. Experts compared the original English version of the scale against the two translated versions and selected the one they considered the most resemblant to English semantics.
Back-translation: back to English of the consensus resulting from the linguistic verification by two Portuguese experts, who did not know about the original scale. The retro-translated scale was then compared against the original version.
The final accepted version of the PHQ-4 scale (in European Portuguese) was then applied to a subset of 46 convenience participants from the general population (n=29) and GP/FMD (n=17), aiming to evaluate its understandability, internal consistency, and reliability. Informed consent was recorded.
All participants were asked to answer a questionnaire which, in addition to the PHQ-4 scale, also included a list of context questions related to gender and age group.
Participants responded to the questionnaire at two different time points, in a test and retest format. Initially, participants were asked to respond to the questionnaire in a written format, followed by a second moment where the same questionnaire was applied orally by the investigator who collected their answers. There was an interval of, at least, 15 minutes between both evaluation time points, as a measure of reliability.
During the validation phase, an observational and correlational study was conducted with GP/FMD specialists and internees practicing in Health Centre Groups (Agrupamentos de Centros de Saúde, ACeS) under the management of the RHA of Central Portugal, who voluntarily accepted to be part of the study, to co-validate the PHQ-4 scale with the EQ-5D-3L scale and the “Sentimentos Negativos - Negative Feelings” sub-scale (part of the SoGeMM-MGF scale).
GP/FMD Portuguese specialists and trainees in the Portuguese National Health System can work in one of three kinds of primary healthcare units: Personalised Healthcare Unit (UCSP), Family Healthcare (model A, USF-A), and Family Healthcare (model B, USF-B), which differ in how they are structured and how they manage the list of patients being followed up. Portuguese National Health Service defines, as a decentralised entity, the Administração Regional de Saúde (RHA) and, subsequently, the Agrupamentos de Centros de Saúde (HCG).
The protocol for data collection was approved by the Health Ethics Commission of the RHA of Central Portugal and the permission for using the scales mentioned above has been authorised by the respective authors.
Study participants were enrolled from GP/FMD-related social media groups, due to the COVID-19 pandemic, using an invite shared by the investigators. This invite provided a link to the server where the questionnaire had been hosted. Only one invitation was made. The questionnaire included an introductory section with an informed consent request, which is necessary for the answers to be accepted and validated. Throughout the process, the confidentiality and secrecy of the participants have been assured. In addition to the three instruments mentioned above, the questionnaire also included a set of questions to evaluate the context characteristics of the population: gender; age group; place of work (unit); career stage (internee vs specialist), and, if specialist, trainer on its or a different specialty and HCG of work.
Data collection took place between July and September 2020.
After data was collected, descriptive and inferential statistics were used. With that in mind, the 25th edition of the Statistical Package for the Social Science (SPSS) was used, with a P value of <0.01 for statistical significance. Descriptive and inferential statistics, non-parametric Mann-Whitney U; Kruskal Wallis Tests, Cronbach’s alfa if item-deleted, and F-test were used, based on the type of variable studied.
Tools
PHQ-4
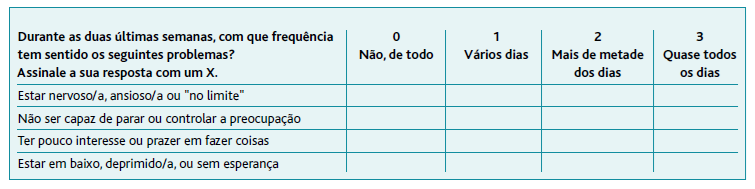
PHQ-4 is a four-point Likert-type scale that evaluates how often the respondent was affected by different problems over the two weeks before the questionnaire. A score of 0 to 3 is attributed to each item (0 - Not at all; 1 - Several days; 2 - More than half the days; 3 - Nearly every day). This screening tool comprises two subscales: Anxiety/GAD-2, consisting of items 1 and 2, and Depression/PHQ-2, consisting of items 3 and 4. The total score is determined by adding together the individual scores of each of the four items, which can range between 0 and 12, allowing to classify the levels of distress in four categories: none (0-2), mild (3-5), moderate/’yellow flag’ (6-8) and severe/’red flag’ (9-12). By applying the subscale GAD-2, a result of 3 or more in the sum of the scores of the first two items suggests anxiety. In the same way, a score ≥3 in the PHQ-2 subscale identifies the individuals who may be affected by this problem. Scores >5 on any subscales should be considered ‘red flags’. For clinical use, the authors recommend considering the sum of the scale, followed by the individual study of the subscales for anxiety and depression. (12-13
EQ-5D-3L
EQ-5D-3L is a tool for health-related quality-of-life assessment. It consists of a descriptive system that allows for the characterisation of the respondent’s health state through five different dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each of these dimensions can be described using a three-level severity scale, corresponding to ‘no problems’ (1), ‘some problems’ (2), and ‘extreme problems’ (3), respectively. (17 The responses to the descriptive system can then be aggregated through a society value-sensitive algorithm, resulting in a value index that can be used to compare the health state of the respondent with one of the populations where they belong. For the Portuguese population, the estimated average of the utility score is 0.758. (18
SoGeMM-MGF
SoGeMM-MGF is a questionnaire aiming to assess the burden caused by the management of multimorbid patients, from a medical perspective. It comprises a total of four subscales, but only the subscale “Sentimentos Negativos - Negative Feelings” was used in this work. This subscale includes five self-assessment questions for Likert response, with five options for response each. For every item, the score ranges from 1 to 5 - the bigger the score, the higher the level of burden. (5
Results
After the initial process, the final European Portuguese version of the PHQ-4 scale was obtained (Table 1). This was applied to a sample of 46 individuals (27 from the general community and 19 doctors), with 23 (50.0%) women, 18 (39.1%) aged between 18 and 34 years old, 16 (34.8%) aged between 35 and 64 and 12 (26.1%) aged 65 or over.
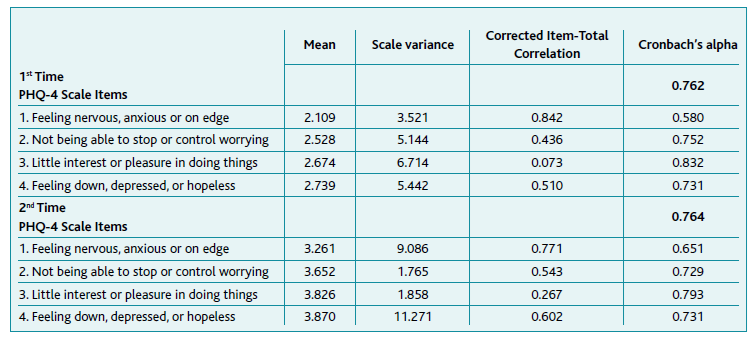
The application of the PHQ-4 scale for the first time led to a Cronbach’s alpha of 0.762, with a Cronbach’s alfa if item-deleted ranging from 0.580 (item 1) to 0.832 (item 3), with a F-test value of 23.224 (p<0.001) and an Intraclass Correlation of 0.762. In terms of the internal consistency at the second time of application of the scale, the Cronbach’s alfa obtained was 0.764, with a Cronbach’s alfa if item-deleted ranging from 0.651 (item 1) to 0.793 (item 3), the Intraclass Correlation of 0.637. These data are detailed in Table 2.
Using the Wilcoxon test to compare the answers between the two-time points, p=0.317 was obtained for «Feeling nervous, anxious or on edge», p=0.100 for «Not being able to stop or control worrying», p=0.317 for «Little interest or pleasure in doing things» and p=0.100 for «Feeling down, depressed, or hopeless».
PHQ-4 mean total scores were not statistically different based on gender (p=0.266) and age (p=0.605).
During the validation phase, a sample of 91 GP/FMD specialists and internees practicing in HCG under the coordination of the RHA of Central Portugal was studied, based on how the application of the questionnaire had been conducted.
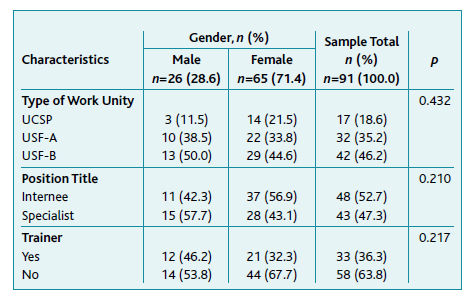
In this convenience sample, 28.6% (n=26) were male and 78.9% (n=71) were younger than 45 years of age. Furthermore, 18.7% (n=17) of the participants worked at the UCSP, 35.2% (n=32) at the USF-A, and 46.2% (n=42) at the USF-B. Of the 43 specialists who responded to the questionnaire, 33 (76.7%), were trainers on their or for a different specialty and the majority of these were women (n=21; 63.6%). There were no statistical differences obtained based on gender (p>0.01) as shown in Table 3.
Using the PHQ-4 scale and given the cut-off limit of 3 in the sum of the GAD-2 subscale, 20.9% (n=19) of doctors had a positive screening for anxiety. In terms of depression, 13.2% (n=12) of participants had a positive screening. As for the levels of distress, the majority of respondents (64.8%, n=59) were not affected by this problem, while 23.1% (n=21), 8.8% (n=8), and 3.3% (n=3) showed mild, moderate and severe distress, respectively. According to Table 4, these results did not show significant gender differences (p>0.01).
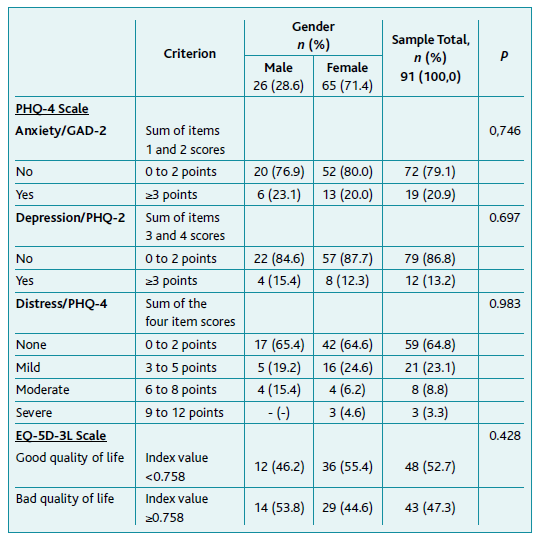
Based on the responses to the EQ-5D-3L scale, 52.7% (n=48) of doctors exhibited an index value lower than the one of the general population (0.758), suggesting a good quality of life. Among male participants, 53.8% (n=14) showed worse quality of life. Female participants (55.4%, n=36) presented a good quality of life. These results did not show significant gender differences (p=0.428). More detailed data can be found in Table 4.
Regarding the “Sentimentos Negativos - Negative feelings” subscale of the SoGeMM-MGF scale, the Kolmogorov-Smirnov revealed no normal distribution of its numerical score (Lillefors correction p=0.004).
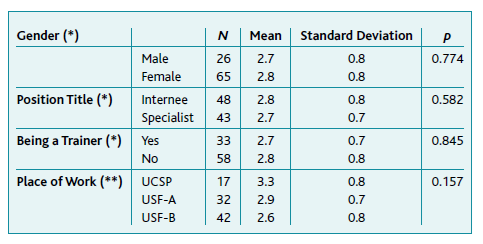
Although not significantly different, the mean value of response to the subscale was higher in female GP/FMD, specific training internees, non-trainer specialists (either in their or other specialty), and among doctors working in UCSP, suggesting a greater burden of negative feelings, as shown in Table 5.
Table 5 Descriptive statistics of the “Sentimentos Negativos - Negative feelings” subscale (part of the SoGeMM-MGF scale)
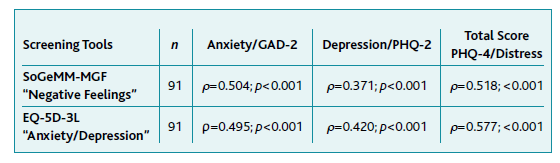
The calculations of the Spearman correlation between the PHQ-4 scale and its subscales, and the other two instruments in comparison are shown in Table 6, with moderate highly significant correlations (p<0.001).
Discussion
The aim of this work was the cross-cultural adaptation and validation to European Portuguese of the PHQ-4 scale, a compact-size screening tool, that allows the evaluation of the psychic state of an individual, in terms of anxiety, depression, and distress, in a timely and effortless way. To achieve this, the work was divided into two stages: cross-cultural adaptation and validation.
In a two-step work, the translation, verification of linguistic adaptation, and back-translation to English were initially conducted, and the reliability of the PHQ-4 scale was then evaluated. The calculation of the Cronbach’s Alfa was α=0.762 (test), and α=0.764 (retest), matching the expectations. (13 The Wilcoxon test allowed us to understand no significant differences between the responses to each scale item at the first and second times of application, confirming its reliability. After data analysis, no significant differences between the average total scores were found with PHQ-4 based on gender and age. This study’s phase was made with data from a non-medic and a GP/FMD convenience sample and supports the successful cultural adaptation of the scale.
As for the concurrent convergent validity phase, PHQ-4 showed a moderate, highly-significant correlation with the EQ-5D-3L scale (ρ=0.577; p<0.001). This correlation occurs in the expected direction: doctors with higher PHQ-4 scores, in distress, obtained a higher score in the ‘Anxiety/Depression’ domain of the EQ-5D-3L scale as well. The subscales PHQ-2 and GAD-2 also showed a positive and significant correlation with the EQ-5D-3L scale. Additionally, there was a moderate correlation between the PHQ-4 scale and the SoGeMM-MGF tool (ρ=0.518; p<0.001). Also, when doctors reported greater psychological distress associated with the management of multimorbidity, the PHQ-4 scale allowed them to corroborate this type of results. Since the values obtained are in line with published literature, it is possible to deduce that the use of the PHQ-4 scale may result in an effective and measurable screening for anxious and/or depressive states, which often affect a doctor’s well-being. The PHQ-4 scale can, therefore, contribute as a first step for a more effective approach which should be complemented by the use of more comprehensive scales and/or clinical interviews at a later stage. (19-21
This work was made in the GP/FMD specialty, as it is more directly exposed to multimorbidity in Portugal. The present results mean that the PHQ-4 scale can be adapted to the Portuguese medical GP/FMD population. However, more studies are required to evaluate the potential use of this same scale in other medical specialties, and for both cases probably with random samples.
Conclusion
The Portuguese PHQ-4 version is a valid and reliable scale that allows a quick and effortless evaluation of the psychic status of doctors in the clinical areas of anxiety, depression, and distress. A significant correlation between the score from the PHQ-4 scale, quality of life (EQ-5D-3L), and emotional burden (SoGeMM-MGF) confirms it. These results offer strong support for the validation of the PHQ-4 screening tool in Portugal.
Authors contribution
Conceptualization. LMS, and MR; methodology, LMS, and MR; software, LMS; validation, LMS, and MR; formal analysis, LMS, and MR; investigation, MR; resources, LMS, and MR; data curation, LMS, and MR; writing-original draft preparation, LMS, and MR; writing-review and editing, LMS, and MR; visualization, LMS, and MR; supervision, LMS; project administration, LMS.

