











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
A 22-year-old woman with Fibrodysplasia Ossificans Progressiva (FOP), diagnosed when she was 6 years old, presented with multiple heterotopic ossifications (HO) causing esthetic deformity and significant functional impairment. As a consequence, she relied on third parties for her daily basic routines. The patient suffered severe joint stiffness of the limbs and spine, flexion deformity in the hips, dorsolumbar scoliosis, and bilateral hallux valgus.
Painful nodules were present in the posterior right thigh and homolateral dorsum, interpreted as flare-ups. She also suffered from restrictive respiratory insufficiency due to deformity and stiffness of the thoracic cage. Radiographs confirmed the presence of widespread HO, especially at the vertebral column, thoracic region, hips, and right knee (Fig. 1). Imaging of the feet showed characteristic findings of this disease: bilateral hallux valgus, shortening and distal medial protuberance of the first metatarsal, and monophalangism (Fig. 2A). A similar malformation of the right thumb was present (Fig. 2B). Cervical spine imaging revealed tall and narrow vertebral bodies with bridging ossification of the posterior elements and fusion of the facet joints (Fig. 3). Additional findings included shortened and broad femoral necks and osteochondromata in proximal tibias.
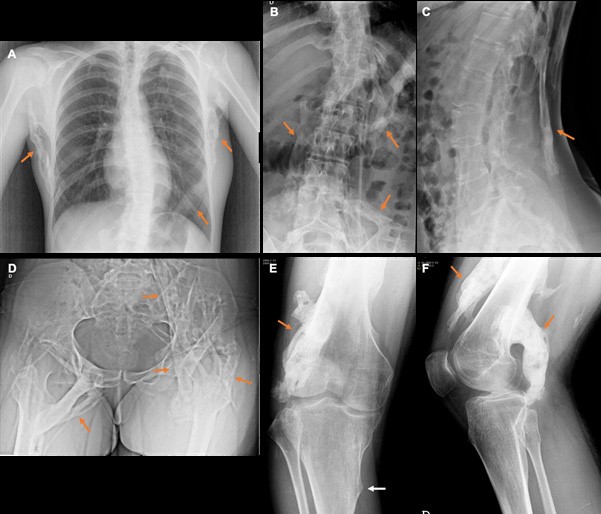
Figure 1: Radiographs show the presence of widespread HO (orange arrows) involving the soft tissues of the thoracic region (A), vertebral column (B and C), pelvis and hips (D), and right thigh and knee (E and F). White arrow in image E depicts osteochondroma in proximal tibia. Dorsolumbar scoliosis is also evident.

Figure 2: Radiograph of the feet (A) depicts bilateral great toe deformities, including shortening and distal medial protuberance of the first metatarsal (white arrows), and segmentation anomaly/ synostosis of the interpha- langeal joint, resulting in monophalangism. Radiograph of the hands (B) also shows a similar malformation of the right thumb (arrow), with clinodactyly and distal medial protuberance of the first metacarpal and proximal phalanx. A dysmorphic distal left ulna is also present.
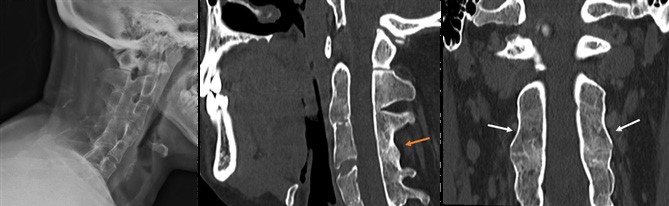
Figure 3: Imaging of the cervical column shows tall and narrow vertebral bodies with bridging ossification of the posterior elements (orange arrow) and fusion of the facet joints (white arrows).
FOP is an extremely rare and severely disabling genetic disease, characterized by congenital malformations of the great toes and progressive HO throughout the body. It is an autosomal dominant disease with an estimated prevalence of 1 per 2 million. The average age of onset of HO is 5 years old (ranging from 6 months to 13 years) and the prognosis is poor (life expectancy of approximately 40 years).1,2,3 FOP most commonly results from spontaneous mutations of the Activin receptor type IA (ACVR1)/ ALK2 gene, classically a heterozygous mutation of a guanine to adenine at position 617 (c.617G>A), with a consequent gain of function. ALK2 binds bone morphogenetic proteins (BMPs) and induces heterotopic bone formation in skeletal muscle, tendons, ligaments, fascia, and aponeuroses. The hard tissue formed represents normal bone and is metabolized via the same process that is observed in normal skeletal tissues.
The most characteristic feature of this disease is HO of the soft tissues that ultimately leads to extra-articular ankyloses. These ossifications have a characteristic anatomical and temporal pattern of progression: axial to appendicular; cranial to caudal; proximal do distal; dorsal to ventral. Typically, the disease progression is episodic, often preceded by minor trauma, iatrogenic interventions or immunological triggers (such as infections). These triggers cause soft tissue swellings and painful nodules (flare-ups), that appear before the formation of ossifications. On imaging, flares appear as swellings of the fascial planes of the muscles, with hyperintensity on fluid sensitive sequences in magnetic resonance imaging (MRI) and marked contrast enhancement, reflecting inflammation and neovascularity (Fig. 4). Malformations in the great toes are present at birth in more than 90% of patients, before the onset of HO. Imaging findings of the feet show bilateral hallux valgus, with distal medial protuberance of the first metatarsal, and segmentation anomaly or synostosis. Similar malformations of the thumbs with clinodactyly can be observed. Vertebral abnormalities are also common, especially in the cervical spine, including tall and narrow vertebral bodies, enlarged posterior elements and variable degrees of facet fusion. Additional findings include delay in skeletal maturation, pseudarthrosis, exostosis, shortened and wide femoral necks, and also extra skeletal manifestations (e.g. central nervous system demyelination).
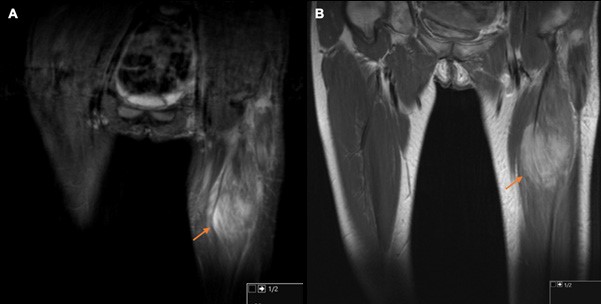
Figure 4: MRI shows an example of a flare in the same patient. Coronal STIR (A) and T1 post-contrast images (B) demonstrate hyperintense signal and contrast uptake in the muscles of the anterior compartment of the left thigh (arrows), especially in the rectus femoris muscle. MRI is very sensitive for the detection of flares in FOP, which may precede the development of heterotopic ossification.
Clinicians often fail to associate rapidly developing soft tissue swellings and malformed great toes to FOP.3 As a consequence, FOP is commonly misdiagnosed as aggressive juvenile fibromatosis, lymphoedema or soft tissue sarcomas. The recognition of the features of this disease is important, because FOP patients are exceptionally sensitive to trauma. Unnecessary surgeries and biopsies are harmful and trigger additional flares.1,2 Treatment is focused on prevention and symptoms support, including anti-inflammatory medication (e.g. steroids) for controlling flares. The most common causes of death in FOP patients are cardiorespiratory failure due to restrictive lung disease and pneumonia.3

