











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
The aging of the Portuguese population, the increased incidence of chronic diseases, and long-term health problems have been determining significant changes in society. Therefore, it is necessary to generate responses that mobilize the different existing resources to meet these people’s needs 1. This is probably a reality that covers many countries, especially in Europe and North America.
We can add a concern from the end of the 20th century or the beginning of this century that the empowerment of citizens must be assumed by nurses as a priority. “Health promotion and disease prevention are two fundamental and transversal axes at all levels of health care provision” 1 (p. 5). Nurses need to acquire skills and develop management competencies that allow them to overcome these challenges.
Also, and this could be our third presupposition, the participation of people in health decision-making is currently presented as a central theme in health policies. This is supported by the belief that people’s involvement and empowerment are essential to improve health outcomes. Starting from this aim, “… it is necessary to mobilize local communities for the protection and promotion of their health, through local health strategies, widely participated. To this end, it is important to invest in each citizen’s ability to make informed decisions about their health, throughout their life course” 2 (p. 8).
Anchored in these three assumptions, about long-term health problems, the role of nurses in empowering citizens, and the involvement of people in health decisions, starting with their own, draws a working horizon in which we inscribe the personalized care planning. In Portugal, the National Health Service’s Person-Centered Care states that support for self-care is based on partnership and working between the individual and the caregiver in a continuous process of communication, negotiation, and two-way decision-making, where both parties contribute to the care planning process to achieve the best possible outcomes for the person 3.
Personalized care planning “…is a collaborative process used in managing chronic health conditions in which people and health professionals identify and discuss problems caused by or related to the person’s health condition and develop a plan to address them.” It further suggests that it be developed through “… a conversation, or series of conversations, in which they jointly agree on goals and actions for the management of the person's health condition” 4 (p. 1).
Personalized care planning is a tool intended for people with various health problems to manage their health care. It allows them to record, in partnership with the health professionals who accompany them, the current situation and the goals set for a certain period, thus sharing the work and responsibility among all the commitments involved in this process. Personalized care planning allows monitoring of the actions and behaviors agreed upon to achieve these goals and evaluates the results reached 2.
Personalized care planning in Portugal is based on the use of the technology provided in the National Health Service Portal; alternatively, when justified, other digital or non-digital support can be used if the first is not available. This plan requires the nurse to monitor the records, the result of the planned actions, and the regular evaluation that each person performs in its implementation 5. Therefore, these aspects embedded the concept of “good management,” in health care planning and implementation, related to goals, monitoring (also the accorded metrics), interventions, and continuous assessment.
Materials and Methods
To identify and describe the evidence on the management of personalized care planning in people with multiple long-term health problems in the community, we conducted a literature scoping review using the Joanna Briggs Institute methodology 6. The project is registered in the OSF Registries database, available at osf.io/5uwpt or in DOI https://doi.org/10.17605/OSF.IO/5UWPT.
Review Question
The questions that guided the research and which were intended to be answered were as follows:
What are the nursing interventions in managing personalized care planning in people with multiple long-term health problems in the community?
What are the strategies used by nurses in the good management of personalized care planning in people with multiple long-term health problems in the community?
Does the good management of personalized care planning by nurses produce health gains in people with multiple long-term health problems in the community?
We have followed the population, concept, context. Population refers to adult people - a person who has reached total growth or maturity. Adults are 19-44 years old, with multiple long-term health problems; concept refers to the importance of understanding the nurse’s management of personalized care planning; context relates to nursing care in the community.
Inclusion and Exclusion Criteria
The search included all types of published studies, available in full text, in which the participants are adults, with chronic disease or long-term health conditions, of both genders, where the intervention included collaborative planning in supporting the self-management of the person’s health problems (between the person and the nurse), in the period from January 1, 2016, to May 31, 2021, in English, Spanish, and Portuguese. Exclusion criteria included studies of adults with dementia, intellectual disability, or communicable diseases, and studies with multidisciplinary teams in which a nurse was not identified as a member.
Search Strategy
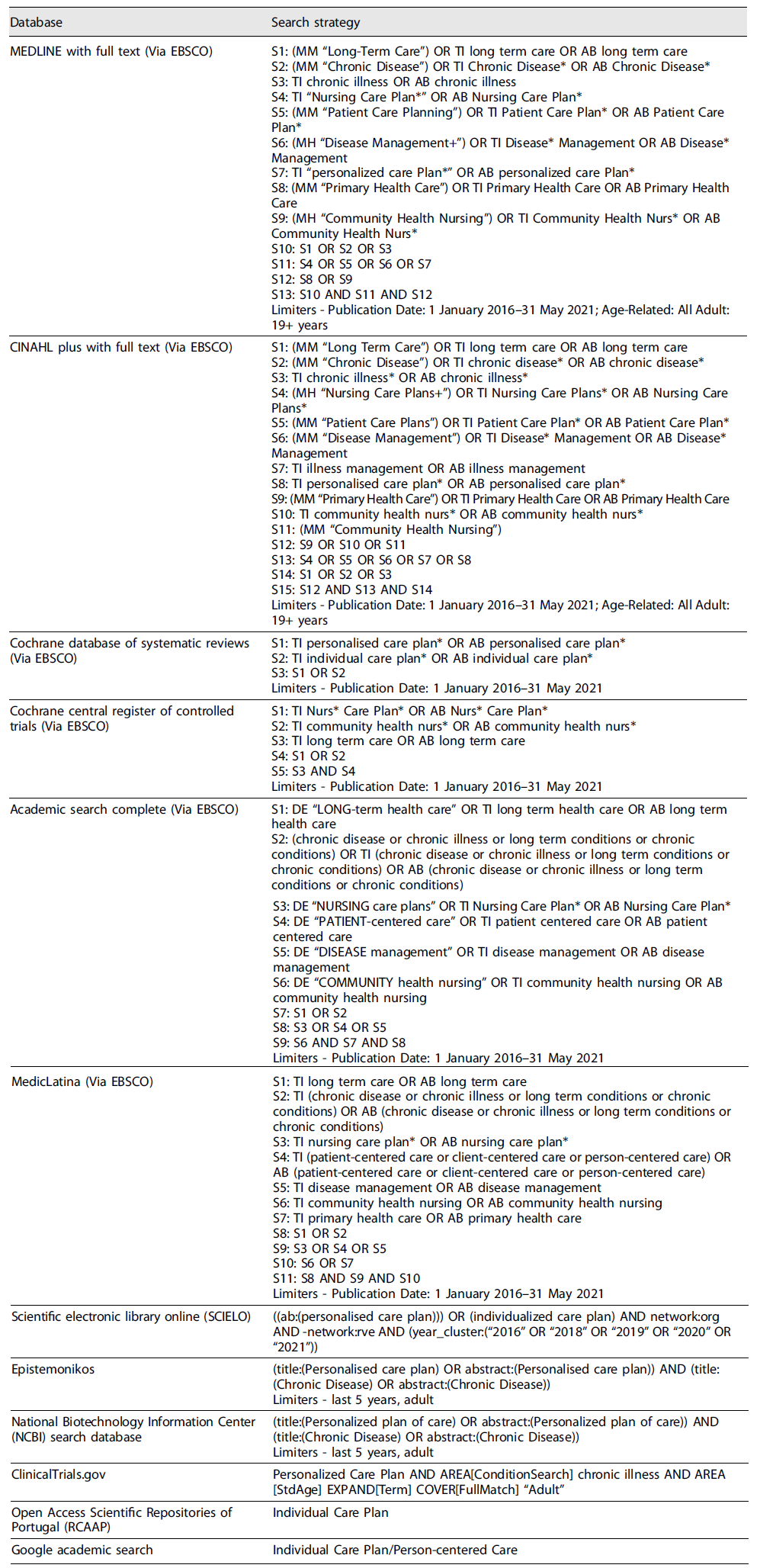
The search strategy was carried out in platforms and databases: Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Medical Literature Analysis and Retrieval System Online (MEDLINE), Academic Search Complete, MedicLatina (Via EBSCO), no - Portugal Open Access Scientific Repository (RCAAP), ClinicalTrials.gov, Epistemonikos, National Biotechnology Information Center (NCBI) search database, Scientific Electronic Library Online (SCIELO), a manual search was made using the Google Academic Search tool, and indexed controlled vocabulary from each database was searched. Articles in which the research participants were adult participants (19-44 years) of both sexes, suffering from chronic diseases, in which the intervention includes a collaborative plan that supports self-management of the person’s health problems, and in which the different contexts of care provision were considered, namely, primary, or continuous health care were included. The search formulas were adapted to each database as shown in Table 1.
Selection of Studies
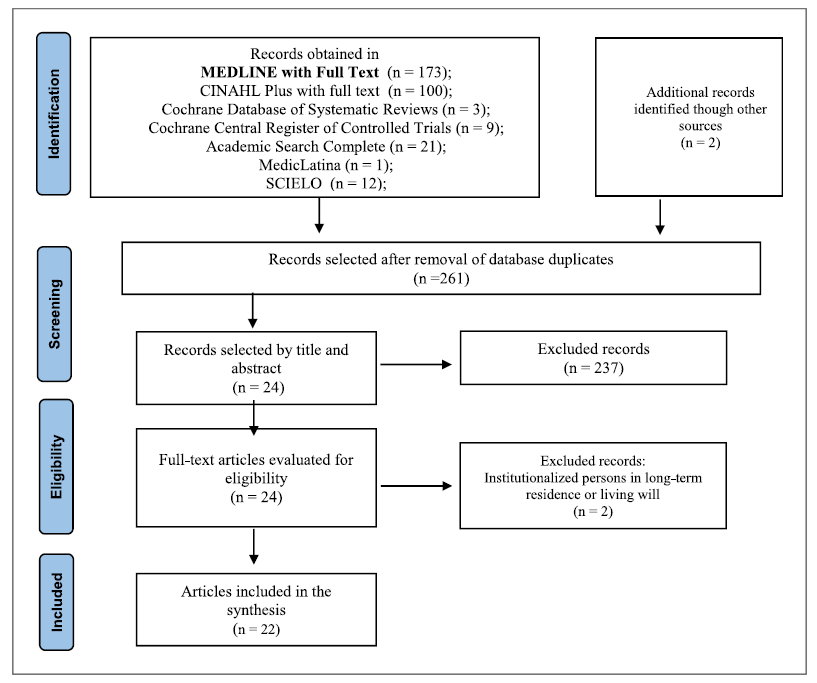
Based on the strategy described, 158 articles were accessed through scientific databases and online repositories: MEDLINE® (n = 173), CINAHL® (n = 100), Cochrane Database of Systematic Reviews® (n = 3), Cochrane Central Register of Controlled Trials® (n = 9), Academic Search Complete® (n = 21), MedicLatina® (n = 1), SCIELO® (n = 12), and Google Scholar, making a total of 321 articles. Sixty duplicate articles were excluded. After applying the inclusion and exclusion criteria, and reading the title and abstract, 237 articles were rejected, and 2 articles were also excluded after their full reading due to the context of the investigation. A total of 22 articles were analyzed, as shown in Figure 1, showing the process of search, exclusion, and selection of the studies found. The PRISMA flow diagram is shown in Figure 1 for scoping reviews according to Joanna Briggs Institute, which identifies the stages of the search performed until the final number of articles to be included in this scoping review.
Results
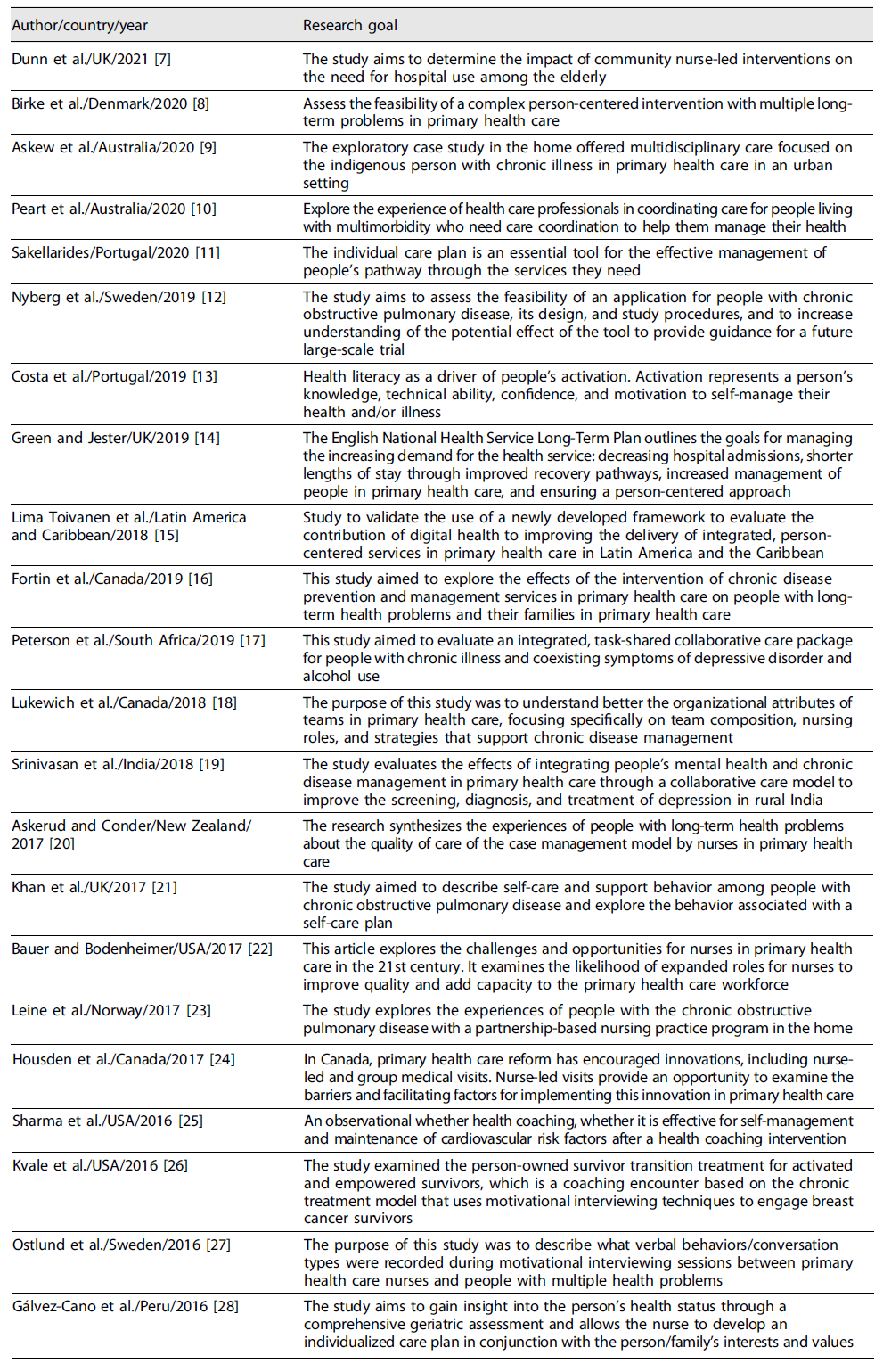
We obtained 22 studies described in Table 2, and the data extraction process was performed according to the methodology for scoping reviews developed by the Joana Briggs Institute. Two reviewers extracted the data independently. The interpretation of the results was based on the questions that guided the research, so we presented them with a summary of the main characteristics and objectives.
Discussion
When assessing the impact of good, personalized care planning management on health outcomes in people with multiple long-term health problems in the community, three questions arise: what nursing interventions, what strategies nurses use, and what production of health gains. The nurses’ intervention focuses on the prevention and management of chronic disease. They support the empowerment of people for self-management of long-term chronic illness, therapeutic adherence, maintenance of health status and quality of life, and use of health services. As negative aspects, they report that people needed a more extended follow-up period to maintain motivation and knowledge acquisition 16.
The nurse’s intervention is based on the management of the care plan with the person, from assessment, counseling, teaching, and support in the informed decision 18, in the identification of cases, to monitoring throughout the person’s progress, with referral to the multidisciplinary team 19. The nurse’s action with the person with long-term problems can also have interventions 7,19,23,26: the empowerment of the person for self-management of their long-term health situation, the support to the person in establishing goals and a plan to improve their health, the promotion of motivation and confidence for self-management, the discussion to identify modifiable behavioral risks and information so that the person can make their choices, the support in self-management, and increase the person’s capacity to manage (self-management) their long-term health situation.
Self-management support programs should be collaborative between health professionals and the person to help them acquire skills to understand and manage their therapeutic plans and disease exacerbations, enable them to adopt healthier behaviors, and manage the socio-emotional consequences of the disease more effectively 21. Involving the person in the individual plan is a significant challenge for health care professionals managing long-term health conditions 21.
Nurses can use health coaching to engage people in self-management of their long-term health problems 25. It is emphasized to promote coaching and training of the person to improve health behaviors and adherence to the therapeutic plan for people with chronic health conditions 23.
As for the work methodology, case management by the nurse enhances the empowerment and follow-up of people with long-term problems, associated with access, response time, availability, trust, and communication. These are attributes valued by people 20.
The nurse should also encourage and empower people to be active participants in their health and with the teams for the co-construction of the collaborative care plan centered on the person, with the definition of their objectives, goals, priorities, and purpose of their health and well-being 9,24, and should promote negotiation 8,11. The nurse is expected to strengthen the person’s motivation and commitment to behavior change, which involves partnership, acceptance, compassion, and evocation, shaping the conversation with the person to evoke and commit the person to behavior change 27 through motivational interviewing 10,14.
Nurses should help people control their health problems by recognizing them and understanding their role and the importance of communicating and collaborating with people in their health management 10,13. The nurse thus assumes the role of a long-term care manager who shares care with the multidisciplinary team in meeting the needs of people with long-term health problems, assuming leadership of these specialized teams for managing people with multiple long-term complex health problems 7,22.
Primary health care nurses support people in navigating the health care system and services, act as a point of contact as people complete their care plan, link them to an evaluation of their plan, and support self-management 10. The nurse uses individualized, personalized responses according to the needs of each person with multiple long-term health problems as a strategy 16.
Nurses also use the process of systematic management and follow-up of people with multiple long-term health problems 18 through the definition of individualized/personalized plans, and information about healthy lifestyles 21. Strengthening communication skills so that nurses place the person at the center of care allows for developing communication pathways and referrals for community support 17,27.
The nurse also uses health coaching to manage long-term health problems in the community (follow-up/coaching between 12 and 24 months) 25 or uses coaching based on the chronic care model that uses motivational interviewing techniques to empower people 26.
Case management is centered on people with long-term health problems in the community, with an emphasis on education, self-management, and collaboration, so that people can manage their health condition 20 - the responsibility is shared between nurse and person to improve outcomes for health conditions such as diabetes and hypertension 22. This practice is based on centered, individualized, personalized partnership between the nurse and the person with multiple long-term health problems 8,9,23, with the support of multidisciplinary nurse-led community teams 7,24.
Person-centered practice is fundamental to evidence-based nursing practice, establishing a partnership with the person and respecting their wishes, adapted to their specific needs and preferences 10. Optimizing the provision of person-centered nursing care involves community-based nursing care; keeping the person with multiple health problems at home favors the prevention of hospital admission as well as shortening the length of hospital stay, if necessary; partnership with people is at the center of care delivery throughout the National Health Service 14.
Comprehensive geriatric assessment can enhance a multidimensional and interdisciplinary diagnostic tool that assesses the person’s health in all its complexity 28. It is worth mentioning the use of IT tools such as a digital application to support people with chronic obstructive pulmonary disease, co-created with nurses 12, or the digital application eHealth to support the management of health problems of people with multiple health problems 15 in a personalized care planning based on an information system as a challenge of multimorbidity.
Health literacy should be used as a driver of people’s activation. Activation represents a person’s knowledge, technical capacity, confidence, and motivation to self-manage health and/or disease 13 effectively motivating individual paths and managing essential instruments for the effective activation and management of people’s path through the services they need, through shared decisions throughout the care process and effective communication 11.
The health gains in people with multiple long-term health problems in the community, perceived as positive, were grouped into six major themes: awareness; improved knowledge; better motivation and empowerment; adoption, of healthy enhanced behaviors; improved health status; and improved quality of life 18. Among these, the first three are identified as intermediate gains, since they contribute to the achievement of the other three, considered as, final gains - the adoption of healthy behaviors; improved health status enhanced quality of life. There are also gains in family members, according to their involvement, changing health behaviors 16.
Nurses provide a set of services that have the potential to produce gains in people with multiple long-term health problems, even without the support of an interdisciplinary team. A nurse makes profit gains when they are present in the multidisciplinary team, as in the control of hemoglobin A1c, fasting glycemia, blood pressure, and cholesterol in people with diabetes 18.
The model of collaborative care between nurses and the person with multiple long-term health problems shows significant gains, allowing 40% of the participants in the control group to recover, allowing the identification of 2.1 more cases of people with mental illness and multiple long-term health problems, also allowing the linking of community members to primary care, increasing awareness of mental health in the community, and reducing the stigma of mental health 19. It also allows for health gains through identifying and managing the health status of people with mental illness, and other comorbid conditions, by nurses, and a reduction in depressive symptoms through nurse’s value of identification and treatment by the nurse was predictive and positive for both depression and alcohol disorders 17.
Having a collaborative self-management plan was positively associated with adherence to the therapeutic plan, greater knowledge of the disease, increased participation in training and support groups as well as the quality of life; collaboratively, nurse interventions to support patient self-management reduce the need for hospitalization for respiratory cause and improve quality of life 21. Maintaining the person in a nurse-managed health “coaching” program over time enhances the person’s health goals 17.
Case management increased self-confidence, promoted self-management of long-term health problems, and increased quality of life; having access to nurse case managers who were good communicators was also significant 20,22,26 and decreased the use of health care 7,14,23. Co-goal setting and care planning focused on people with multimorbidity and reduced nurses’ workload 8. It also promotes health status maintenance and improved health status perception by people with multiple long-term health problems as well as decreased rates of depression 20. It provides greater knowledge and understanding of people and health care professionals and greater involvement of health care professionals and increases personal activation 24. Motivational conversation predicts changes in desirable behaviors. Motivational previewing also helps identify symptoms to improve symptom and health management 27.
Health literacy increases people’s confidence and ability to manage their health 13. The co-management of care and the pathways of people with multiple long-term health problems who use health care get the services they need, promptly, with good incomes at the end 11. Based on the interpretation and synthesis of the evidence identified in the personalized care plannings, the results are summarized in Figure 2, mirroring our understanding of what contributes to the successful implementation of the personalized care planning.
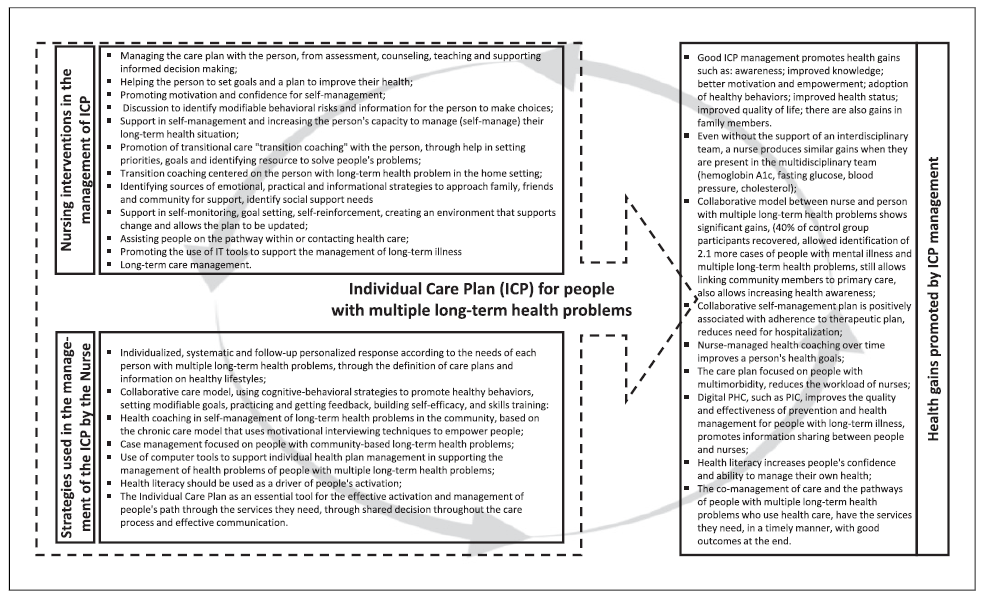
Fig. 2 Summary of nursing interventions, strategies, and health gains in the good management of personalized care planning.
Limitations of the Study
The comprehensive view of personalized care planning and the multiplicity of forms of organization of health systems at a global level may be a limitation to interpreting results. Future research should include an experimental or quasi-experimental methodology to identify the effectiveness and efficiency of specific nurse interventions in personalized care planning. On the other hand, it will be relevant to describe and identify public health policies and their implementation in practices to evaluate their effectiveness. We can consider as limitations the fact that we included studies in three languages (English, Portuguese, and Spanish) and available in full text, which may have reduced the number of studies with potentially interesting results for our subject.
Contributions to Practice
The systematization of evidence on personalized care planning allows nurses to identify interventions and strategies that produce gains in health and savings in nursing care. The success of personalized care planning in people with multiple long-term health problems needs to be systematically managed and evaluated concerning the health gains of the people involved and the nursing care indicators.
Conclusions
Our objectives were to identify and describe the evidence on managing personalized care planning in people with multiple long-term health problems in the community. We conclude the management of personalized care planning allows for a person-centered intervention by nurses; implementing strategies focused on prevention and health management in people with multiple health problems promotes the empowerment of people for self-management of long-term health problems through assessment, management, counseling, teaching, and support for informed decision-making together with the person. Good management of personalized care planning by the nurse promotes health gains in people with multiple long-term health problems.
Author Contributions
The research strategy was defined by both authors; it was carried out by both authors separately on platforms and databases. The two authors independently extracted data. The interpretation was carried out and evaluated by both so that together they present the results with a summary of the main characteristics and objectives. All authors approved the final manuscript.

