











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
Odontogenic cysts are commonly found in dental practice. They are pathological cavities lined with odontogenic epithelium, classified as developmental or inflammatory. Their genesis is closely related to dental ontogeny. Most of them are formed from odontogenic epithelium or its embryonic remnants.1-3
The dentigerous cyst is the most common developmental odontogenic cyst.1,4,5It arises from the dental follicle of na unerupted tooth, surrounding it and connecting to it by the cementoenamel junction. It is thought to develop due to fluid accumulation between the crown of the tooth and the enamel epithelium. Dentigerous cysts occur most frequently in the posterior mandible. Although they can affect any tooth, they are most associated with third molars. They can also be related to supernumerary teeth or odontomas. These cysts can appear at any age but are more common in individuals between 10 and 30 years of age, with a slight predominance for males and Caucasians.1-6
Dentigerous cysts are mostly recognized during a routine radiological examination or after noticing the delayed eruption of a tooth or even tooth crowding caused by the pressure it exerts.5-7 Clinically, they are slow-growing and asymptomatic, except when infected. Their evolution may lead to clinical complications such as displaced teeth, ectopic eruption, root resorption of adjacent teeth, occlusal problems, facial asymmetry due to bone cortical expansion, and even malignancy.8
Radiographically, the dentigerous cyst appears as a unilocular radiolucent lesion with well-defined margins involving the crown of a tooth.1,5,9-11 However, these imaging methods are insufficient to establish a correct diagnosis, and an anatomopathological analysis is always necessary. The differential diagnosis of a smaller dentigerous cyst includes the dental follicle or hyperplastic dental follicle, while that of a larger one includes the unicystic ameloblastoma and the odontogenic keratocyst.12,13
Histologically, the dentigerous cyst presents a loosely arranged fibrous tissue capsule lined by non-keratinized stratified pavement epithelium, with two layers of cubic epitelial cells. In case of inflammation, the capsule is more keratinized and may contain a mononucleated inflammatory infiltrate.
The content of the cyst is a hemorrhagic or serous exudate.1,14,15 The cyst’s dimensions and location, the teeth and structures involved, and the patient’s age and health status are fundamental criteria in the treatment decision process.
The most common approaches are marsupialization or enucleation and extraction of the unerupted tooth. However, if the eruption of the involved tooth is considered possible, it can be left in place after the partial removal of its capsule.16
Despite being non-neoplastic, the dentigerous cyst has a neoplastic potential. Thus, if it goes unnoticed or is not completely removed, its epithelial lining may start developing benign or malignant tumors. Adequate treatment has an excelente prognosis, and recurrence of the lesion is rare.2,5,14 Gathering all relevant information and accurately diagnosing the dentigerous cyst is crucial for its effective treatment. Yet, as other lesions appear alike radiographically, na anatomopathological exam is mandatory for a definitive diagnosis.1,5,17,18
This investigation aimed to assess the prevalence of dentigerous cysts in a population with bone pathology who attended the consultations of Oral Surgery and Oral Pathology Master’s Degrees at the Faculty of Dental Medicine of the University of Porto (FMDUP), between 2000 and 2023. Additionally, it intended to study the concordance rate between clinical and histological diagnoses within the analyzed bone pathology cases, and characterize the pathology regarding its anatomic location, its association with impaction, and the patients’ age and sex.
Material and Methods
Anatomopathological records of patients with bone pathology who attended the consultations of Oral Surgery and Oral Pathology Master’s Degrees of FMDUP between 2000 and 2023 were selected. Only bone pathology cases were considered.
The data collected comprised age, sex, anatomic location, association with impaction, and the associated tooth. All cases in which clinical information was missing or was too wide-ranging were excluded. Each selected case was subsequently classified into one of three groups: totally concordant when the clinical diagnosis matched exactly the histological diagnosis; partially concordant when the histological diagnosis was one of the options considered in the clinical diagnosis; and discordant when the clinical diagnosis did not match the histological diagnosis.
Descriptive analysis was performed to calculate the prevalence of the dentigerous cyst and its characterization. Furthermore, the concordance rate between the clinical and histological diagnoses was also measured. Data was collected using Microsoft® Excel® (Microsoft Office 365 ProPlus, 2023 version) software.
The statistical analysis of the results was conducted using IBM® SPSS Statistics (version 27). Pearson’s chi-square Independence test was used with a significance level of 0.05 to determine the association between the dentigerous cyst and the patient’s sex and between the dentigerous cyst and its location. The null hypotheses were defined as “The variable ‘dentigerous cyst’ is independent of the variable ‘sex’” and “The variable ‘dentigerous cyst’ is independent of the variable ‘location.’”
The anonymity of all participants was maintained throughout the research process, and the Ethics Committee for Health of FMDUP accepted the project. The entity responsible for the access to the information required -RAI (Responsável do Acesso à Informação)- also accepted the project.
Results
A total of 263 anatomopathological records of bone pathology were consulted, of which 25 cases were excluded due to corresponding to non-pathological changes. Of the remaining 238 cases, 25 included dentigerous cysts, corresponding to 10.50% of all cases of bone pathology. Among the 161 odontogenic cyst cases, the dentigerous cyst prevalence was 15.50%.
The mean age of patients with dentigerous cysts was 36.9 ± 13.5 years old, but three cases had no information regarding the age (Figure 1). Male patients accounted for 68% of the dentigerous cyst cases. The chi-square tests evaluating the association between the cyst and sex revealed that the two variables were independent (p=0.121).
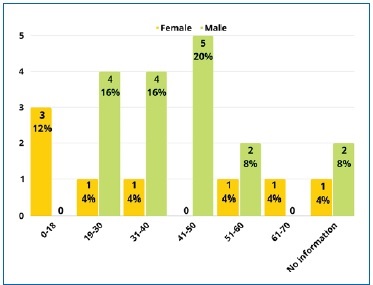
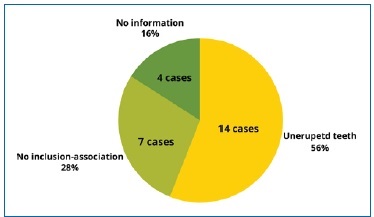
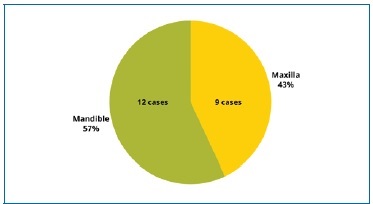
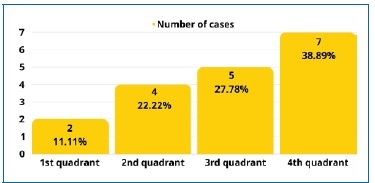
Figure 2 shows the distribution of the dentigerous cyst regarding the impaction of the associated tooth. Four cases had no clinical information on the cyst’s location and were excluded (Figure 3). The chi-square tests evaluating the potential association between the dentigerous cyst and its location among the well-documented 188 bone pathology cases revealed no statistical significance between the two variables (p=0.289) (Figure 4). Three of the 21 cases had no information about the quadrant and were excluded (Figure 5).
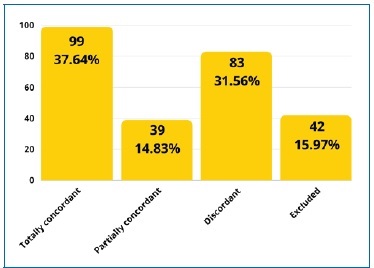
When calculating the concordance rate between clinical and histological diagnoses of the 263 bone pathology, 42 were excluded due to lack of clinical information, reducing our sample to 221 cases. Of these, 62.45% had a correct suspicion of the final diagnosis (Figure 6).
Discussion
Bone pathology is very common in the oral cavity. This study found that the dentigerous cyst had a prevalence of 10.5% in bone pathology cases but a prevalence of 15.5% among odontogenic cyst cases. This prevalence agrees with the results from a South Indian population study (13.4%),19 an investigation by Pedro Vitali Kammer et al. (14.04%),20 and a retrospective study by Paris Tamiolakis et al.21 (14.5%). In turn, this prevalence was slightly higher in an Italian population (23.4%),22 in two different Turkish populations (26.6% and 26.9%),2,23 in an Indonesian population (25.5%),24 and in two Brazilian populations (26% and 27.5%).25,26 Other investigations found much higher prevalence values. A Mexican population reached 41%, which may be related to a higher rate of third molar impaction in this population.3 In two Brazilian pediatric populations, the values were 42% and 44%, probably because only pediatric patients were selected, thus decreasing the number of radicular cysts, unlike in the adult population, where they outnumber the dentigerous cysts. Furthermore, the prevalence was calculated within the whole biopsied oral pathology and not only considering odontogenic cysts.27,28 Finally, a prevalence of 35.3% was obtained at Kuwait University, where the periapical pathology might have been underestimated due to not being always submitted to histopathological analysis.29 Conversely, a substantially lower prevalence of the dentigerous cyst of 1.8% was found in Lebanon, but it was calculated regarding the total of cases and not only individuals with odontogenic cysts or some bone pathology.5
In this study, the dentigerous cyst was more prevalent in male patients, with 68% of the cases. Most of the literature corroborates this prevalence in males over females, including investigations carried out in Italian, Canadian, Lebanese, Mexican, Turkish, and South Brazilian populations, as well as investigations by the University of Kocaeli and Tamiolakis.2,3,5,13,20-22,30 31This prevalence in males has been justified by a reduced jaw size and a greater tendency for prophylactic third molar extraction in women, leading to lower development and prevalence of dentigerous cysts. However, there are no significant differences to suggest that sex is associated with the dentigerous cyst. Thus, the null hypothesis was accepted.
The mean age of the patients diagnosed with dentigerous cysts was 36.9 ± 13.5 years old, with more cases between 19 and 50 years. As in other investigations, the frequency decreased with age, with the highest prevalence between the second and fourth decades of life.
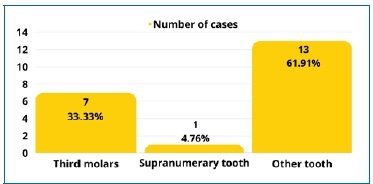
Regarding the dentigerous cysts’ location and associated teeth, 56% were associated with unerupted teeth. Of those with sufficient clinical information, only one was associated with a supernumerary tooth, as in a Lebanese population study,5 and 33% were associated with third molars, mainly the mandibular third molar, as in several studies, including some carried out in Mexico, Lebanon, Turkey, and Canada.2,3,5,12The results also indicated a predilection for the mandible, corresponding to 57% of the cases, which agrees with the literature referred. Moreover, dentigerous cysts were more prevalent in the fourth quadrant (38.89%). However, no significant diferences suggested that location is associated with the dentigerous cyst.
The present study calculated the concordance rate between the clinical and histological diagnoses of bone pathology. In 44.80% of cases, the clinical and histological diagnoses were totally concordant, which provides a reasonable percentage of diagnostic accuracy. Moreover, 17.65% of the cases were partially concordant. Thus, 62.45% of the cases had a correct suspicion of the final diagnosis. In turn, in 37.55% of the cases, the clinical and histological diagnoses disagreed, corresponding to a high error rate. This finding may be due to a lack of rigid standardization of procedures. This high value may also result from the similarity of the cyst with its differential diagnoses, which leads dentists to know that it is mandatory to do a histological analysis and be careless, leaving the diagnosis only to the anatomopathologist’s responsibility. Although a 100% concordance rate was not expected because pathologies may have similar appearances when observed through clinical examination and imaging, this discordance rate must be improved.
It should also be noted that 25 cases that went through histological analysis were excluded due to being non-pathological.
This situation should not be considered a mistake, unlike the 42 cases excluded due to lack of information, and it highlights the importance of the anatomopathological exam to establish a correct diagnosis.
The limitations of this study are the data collected corresponding to an extended period and the non-uniformity of criteria in the diagnoses. Furthermore, this is a conditioned study group, composed only of patients referred to the Oral Surgery and Oral Pathology Master’s Degrees appointments.
In addition, the lack of information conditioned the results and did not allow a more detailed statistical analysis.
It would be interesting that future investigations do a prospective study with strict rules to carry out anamneses and clinical and histological diagnoses. The population should not be restricted, consisting of all patients who attend the FMDUP clinic appointments, a totally randomized population.
It is imperative to have good and complete information regarding the clinical diagnoses. Information about the lesion, the patient, clinical history, and anamnesis should be sent to the anatomopathologist alongside the radiographic image.
Conclusions
The prevalence of dentigerous cysts within bone pathology cases in the population investigated was 10.50%. It was more prevalent in males and the mandible. The cyst had a higher prevalence between 19 and 50 years of age.
The concordance rate between clinical and histological diagnoses was 62.45%, which can and should be improved despite being a high value. This investigation also proves the importance of a correct and complete collection of clinical information and the need to perform an anatomopathological analysis to reach a correct diagnosis.

