











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
Population ageing is a worldwide concern and it is estimated that by the year 2064 adults over 65 will account for 38.7% of the total population (Julio, Clavero, & Soler, 2018). In Europe, the estimated population is 515 million, 19% of whom are 65 or older, and it is expected that by 2060 that number will increase to 29% (Leij-Halfwerk et al., 2019; Observatory on Health Systems and Policies [OECD], 2017). Portugal has ageing rates very similar to the world reality. It is estimated that in the next 50 years the number of older people will triple (Grupo de Trabalho Interministerial, 2017; OECD, 2017). Despite being a natural process, ageing puts the body through several anatomical, functional, biochemical and psychological changes, with repercussions on health conditions. The nutritional status of older adults is one of the dimensions that is often compromised, with malnutrition being one of the most prevalent nutritional disorders in this population (Pereira, Cotta, & Frabceschini, 2006; Santos, Machado, & Leite, 2010; Silva, Marques, Leal, Alencar, & Melo, 2015).
1. State of art
The World Health Organization (WHO) defines malnutrition as deficiencies or imbalances in the intake of energy and/or nutrients (WHO, 2017). According to studies carried out, 60% of the older adults worldwide is in the condition of malnutrition or at risk of it (Damo, Doring, Alves, & Portella, 2018). This condition can lead to an increase of morbidity and mortality, as well as of the susceptibility to infections and a reduction of the quality of life (Silva, Maques, Leal, Alencar, & Melo, 2015). The nutritional status of the older adults must be assessed in a broad and interdisciplinary way, contradicting the beliefs that nutritional changes are part of the normal ageing process (Santos et al., 2010). Thus, the thoroughness of this assessment is essential, which includes parameters related to changes in body composition resulting from the senescence process (Santos et al., 2010). Older adults tend to have a decrease of their weight (loss of bone and muscle mass), a decrease of their height (plantar flattening, decrease of the height of vertebrae and intervertebral discs), and postural changes (Fávaro-Moreira et al., 2011; Santos et al., 2010).
Physical examination, anthropometric indicators, biochemical parameters, bioelectrical impedance and the subjective nutritional assessment are some of the tools that can be used by professionals to complement nutritional assessment (O’Keeffe et al., 2019; Santos et al., 2010). Health professionals who dedicate themselves to caring for older adults in their day-to-day lives have greater practical knowledge about this population (Costa, Cunha, & Oliveira, 2013). Consequently, they play a very important role in detecting problems that may arise from food / nutritional status, allowing them to adjust care and answer the needs of these people with the aim of reducing the risk of malnutrition or improving their nutritional status (Costa et al., 2013).
This way, it is fundamental to carry out a diagnosis of the situation using instruments such as the Mini Nutritional Assessment (Vellas et al., 2006), validated for the Portuguese language as the “Mini Avaliação Nutricional” (Loureiro, 2008), and considered as an excellent monitoring tool. This instrument aims to assess the state of nutrition in older adults and other health conditions, which can lead to a state of fragility. In addition, it helps to identify the population most susceptible to interventions, namely those exposed to risk factors for malnutrition (Carlos, Gazzola, & Gomes, 2016). Therefore, at the same time, it is essential to have a piece of increased knowledge about the risk factors that most often enhance malnutrition in the older adult population.
The older adult goes through a set of changes, which are, in fact, physiological and natural to the ageing process. However, malnutrition is a prognostic factor for health status declining, contributing to greater morbidity and mortality rate. This situation is often under-detected and under-diagnosed (O’Keeffe et al., 2019). In this perspective, the present study aims to identify the risk factors that contribute to malnutrition in older adults.
2. Methods
A systematic review was developed according to the methodology proposed by the Joanna Briggs Institute (JBI) and it sought to answer the following question: what are the risk factors for malnutrition in older adults?
The inclusion and exclusion criteria were selected and the research carried out, followed by the analysis of the studies and data extraction; lastly, a synthesis of the results and a discussion was conducted (Moola et al., 2017).
2.1. Inclusion / Exclusion Criteria
The considered inclusion criteria were studies’ participants being 60 or older and them living in any context (residential structures for older adults and home). The language of the study could be Portuguese, English, or Spanish and no time frame was applied.
2.2. Search strategy
Studies were searched in the databases of the search engines EBSCO, Trip Database, and in the “Repositório Ciêntifico de Acesso Aberto de Portugal” (RCAAP). In the EBSCO search engine, (which includes the respective databases: CINAHL Plus, MEDLINE, MedicLatina, PsycARTICLES, Psychology & Behavioral Sciences Collection, Academic Search Complete), the Boolean equation was used: TI (aged or elderly or senior or older people or geriatric or older adults) AND TI (undernutrition or malnutrition or poor nutrition or under nutrition) AND AB (risk factors); in the Trip Database search engine it was used the Boolean equation: TX (aged) AND TX (malnutrition) AND TX (risk factors); and in RCAAP, using the Boolean equation: TX (elderly) AND TX (malnutrition) AND TX (risk factors);
The research was carried out in December 2019 by one of the reviewers of this study. The selection of the studies was initially carried out by the relevance of the title and / or abstract of the article. This was followed by a complete analysis of the articles with attention to the issue / objective of this review. This process was conducted by two independent reviewers (Moola et al., 2017).
2.2 Data extraction
The data were extracted with focus on the characteristics of the samples, risk factors and typology of risk factors. The divergences found in this process were resolved through dialogue between the reviewers (Moola et al., 2017).
2.2 Summary of the data
The identified risk factors were categorized into extrinsic / intrinsic risk factors. The data are presented in narrative form and using a tabular presentation (Moola et al., 2017).
3. Results
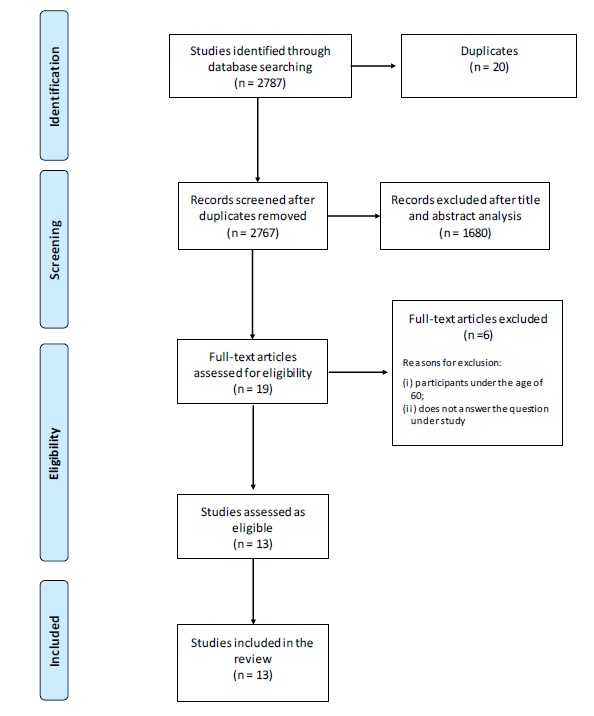
In the research carried out 2787 documents were found, of which 20 were duplicated. After analysing the titles and abstracts, 2748 were excluded, leaving 19 documents for complete analysis. Of these, six were excluded for presenting a sample whose participants were less than 60 years old or for not responding to the study’s question. 13 studies that answered the research question were assessed. For more details see Figure 1 which explains the flow of the selection process.
The 13 selected studies were cross-sectional, descriptive-correlational / analytical studies. The countries of origin of the studies were Turkey (Baz & Ardahan, 2019), The Netherlands (Bakker et al., 2018), Czech Republic (Brabcová et al., 2016), China (Lin et al., 2017), Lebanon ( Boulos, Salameh, & Barberger-Gateau, 2017), Spain (Serrano-Urrea & Garcia-Meseguer, 2013), Mexico (Cruz, Sánchez, & Esteves, 2014), Germany (Smoliner et al., 2009), Korea (Park , Kim, & Kim, 2014), Italy (Donini et al., 2013), Brazil (Ribeiro, Rosa, & Bozzetti, 2011), Greece (Grammatikopoulou et al., 2019) and Portugal (Melo, 2015), with dates of publication between 2009 and 2019.
The participants were inserted in two different contexts: community (Bakker et al., 2018; Baz & Ardahan, 2019; Boulos et al., 2017; Brabcová et al., 2016; Cruz et al., 2014; Donini et al., 2013; Grammatikopoulou et al., 2019; Lin et al., 2017; Park et al., 2014; Ribeiro et al., 2011) and nursing homes (Donini et al., 2013; Melo, 2015; Ribeiro et al., 2011; Serrano-Urr ea & Garcia-Meseguer, 2013; Smoliner et al., 2009).
The 13 studies involved 21568 participants, of which 12860 (59.6%) were female and 8714 (40.4%) were male, with a lower age limit of 60 and an upper limit of 100 years. In the total of the participants, 2349 (10.9%) were at risk of malnutrition and 7796 (36.1%) were malnourished. See Table 1.
Table 1 Characteristics of the participants in the included studies
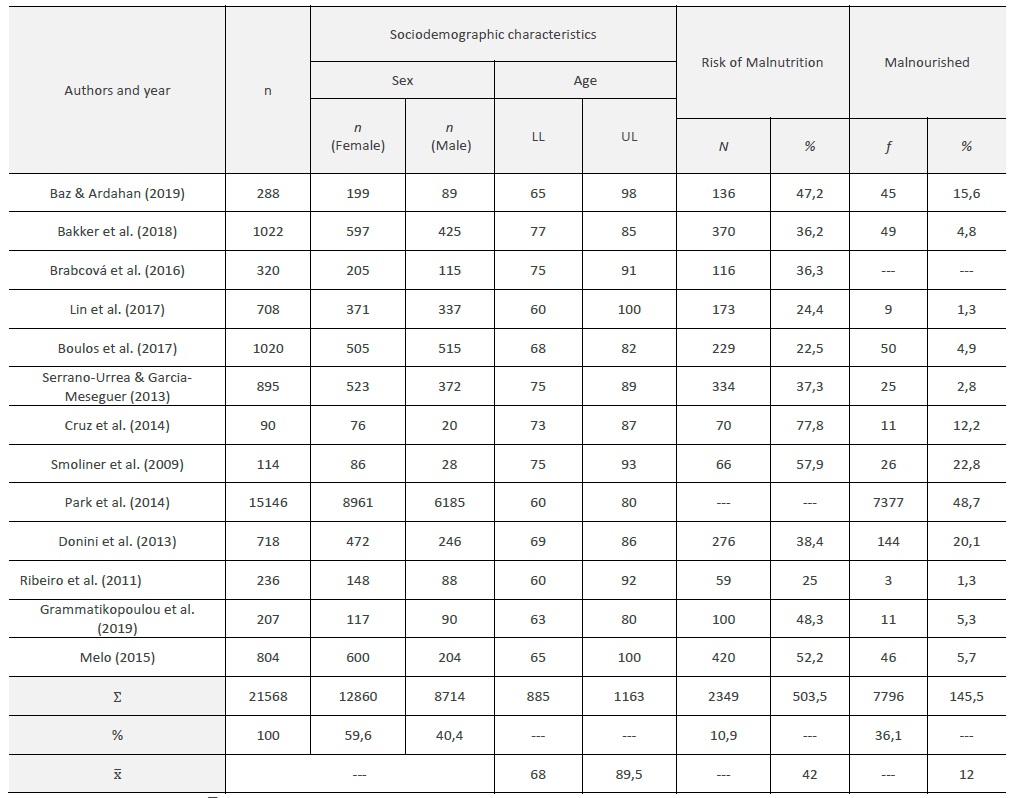
LL: Lower limit; UL: Upper limit; ∑- Total
Source: Elaborated by the author (2020)
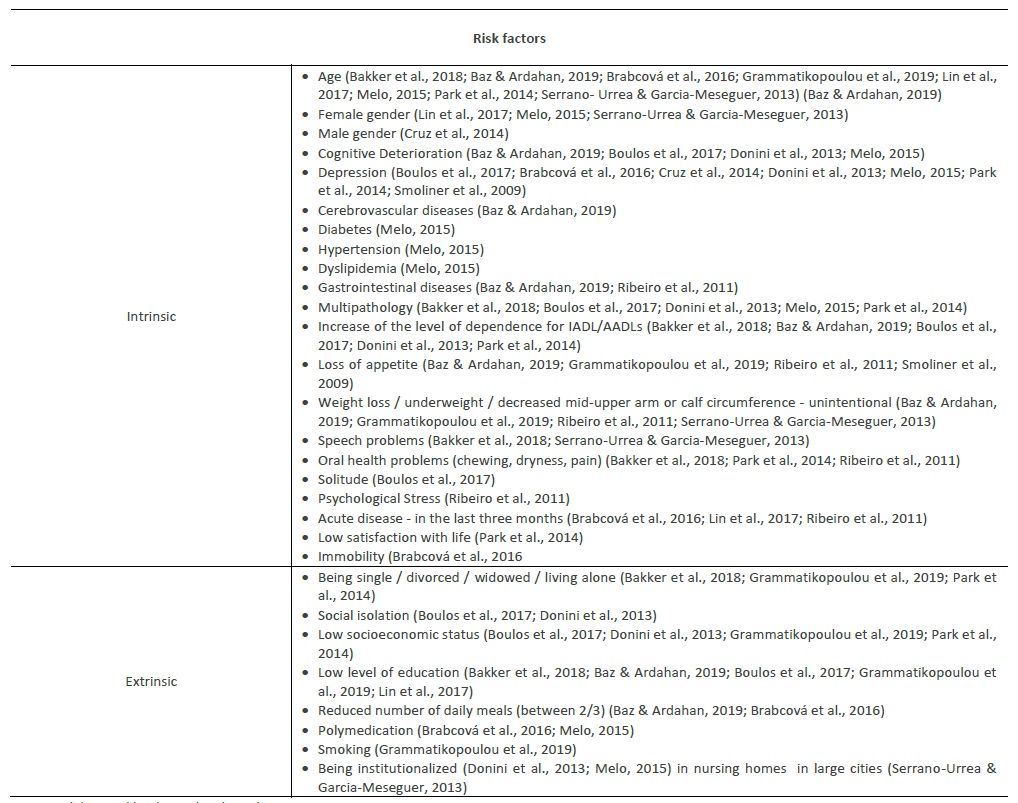
The risk factors identified by the reviewed literature were organized into two categories: intrinsic and extrinsic risk factors. Increasing age, depression, cognitive deterioration as dementia, gastrointestinal diseases and cerebrovascular diseases and some level of incapacitation for instrumental activities of daily living - IADL (such as inability to go shopping and cooking and a greater level of dependence on basic activities of daily living) are some examples of intrinsic risk factors that contribute to the risk of malnutrition (Bakker et al., 2018; Baz & Ardahan, 2019; Boulos et al., 2017; Brabcová et al., 2016; Cruz et al., 2014 ; Donini et al., 2013; Grammatikopoulou et al., 2019; Lin et al., 2017; Melo, 2015; Park et al., 2014; Serrano-Urrea & Garcia-Meseguer, 2013; Smoliner et al., 2009).
In turn, social isolation, low level of health literacy, low level of education, living alone, being single / divorced, low socioeconomic status and being institutionalized are risk factors extrinsic to the individual that deserve to be taken into account when one intends to prevent malnutrition (Bakker et al., 2018; Baz & Ardahan, 2019; Boulos et al., 2017; Donini et al., 2013; Grammatikopoulou et al., 2019; Lin et al., 2017; Melo, 2015; Park et al., 2014; Serrano-Urrea & Garcia-Meseguer, 2013).
4. Discussion
Population ageing has occurred in a context of major social, cultural, and economic changes. In turn, malnutrition is considered one of the most prevalent problems in older adults, which can significantly interfere in the evolution of the health profile of this population segment, regardless of the context (Fávaro-Moreira et al., 2011; O ' Keeffe et al., 2019). Malnutrition used to be studied as a result (consequence) of a comorbidity (e.g.: dementia). However, recent studies emphasize the need for prevention of malnutrition and increasingly explore the risk factors that contribute to this. Possibly, for this reason, the studies found tend to be recent.
Thus, emerges the need for health professionals and all those whose areas of knowledge are linked to the older adults, to know the risk factors of malnutrition and take preventive measures or even, when confronted with these risk factors, intervene or refer it to other health professionals in order to mitigate the evolution of this condition - malnutrition.
Based on this review, it can be seen that of the 21568 participants, approximately 11% were at risk of malnutrition and 36.1% were already in a state of malnutrition. Age and gender were two correlated variables, as older females tend to have a longer lifespan and lower quality of life, while older males tend to live fewer years, but with a better quality (Brabcová et al., 2016; Melo, 2015).
Studies have also found an increase of malnutrition along with the increasing of age (Bakker et al., 2018; Baz & Ardahan, 2019; Brabcová et al., 2016; Grammatikopoulou et al., 2019; Lin et al., 2017; Melo, 2015; Park et al., 2014; Serrano-Urrea & Garcia-Meseguer, 2013); it manifests earlier in the elderly females (65-69 years), while in the elderly males it manifests later (Serrano-Urrea & Garcia-Meseguer, 2013). With regard to bioelectrical impedance, it was confirmed that the elderly males had higher parameters for weight, muscle mass, bone mass, metabolic rate, and visceral fat (Melo, 2015), which possibly function as protective factors for them.
Cognitive deterioration, which includes the various types of dementia, increases the inability to eat, forgetfulness and the inability to recognize the need to eat food, as well as the presence of maladjusted behaviours such as keeping food in the mouth. The older adult with cognitive changes becomes more distracted, slower during meals and more dependent on others to be fed (Baz & Ardahan, 2019; Boulos et al., 2017; Donini et al., 2013; Melo, 2015), requiring special attention from health professionals.
Depression is one of the most mentioned risk factors in the studies analysed (Boulos et al., 2017; Brabcová et al., 2016; Cruz et al., 2014; Donini et al., 2013; Melo, 2015; Park et al. , 2014; Smoliner et al., 2009); these studies describe that the older person, when carrying this condition, shows 3.5 times more weight loss, compared to those who do not have it (Brabcová et al., 2016). In people who live in their own home, depression develops in 7 to 15% of the individuals, a figure that increases to 20 to 30% in hospitalized patients (Brabcová, et al., 2016). The depressive state is often evidenced with the loss of a close person, leading to social isolation/solitude due to limitation of social activities such as meal times, which in turn results in a loss of appetite and, subsequently, weight loss (Baz & Ardahan, 2019; Boulos et al., 2017; Brabcová et al., 2016; Grammatikopoulou et al., 2019; Park et al., 2014; Ribeiro et al., 2011; Serrano-Urrea & Garcia-Meseguer, 2013; Smoliner et al., 2009). In addition, a study links the male gender with the incidence of depression as predictor of malnutrition (Cruz et al., 2014), and it should be noted that the average age of this population was 80.4 ± 6.9 years (Cruz et al., 2014). Deprivation of affection and the institutionalization process induce depression, being one of the manifestations of this condition the loss of interest in eating meals (Donini et al., 2013). Even though the data from this revision do not allow us to determine in which context the risk of malnutrition is higher, prevalence studies show that these clinical conditions are more frequent in hospitalized and institutionalized elders. The decrease of serotonin levels can also be related to the incidence of depression, leading to a decreased food intake (Melo, 2015). Other emotional states such as psychological stress, solitude and low satisfaction with life are risk factors to be taken into account (Boulos et al., 2017; Park et al., 2014; Ribeiro et al., 2011).
The synergetic effect between the loss of intrinsic capacity and the increase of functional dependence influences how the elderly person accesses food or how they eat. The level of dependence for IADL / ABVD is referred to as being proportional to the risk of malnutrition - as the older person's dependence increases, more difficult it becomes for them to acquire food and cooking and/or eating it (Bakker et al., 2018; Baz & Ardahan, 2019; Boulos et al., 2017; Donini et al., 2013; Park et al., 2014).
Oral health problems such as changes in chewing are part of the ageing process. Most elderly people have a partial or total absence of teeth due to dental cavities and periodontal diseases, thus decreasing the ability to chew and conditioning the choice of food; then, the risk of food becoming monotonous and limited emerges, with a possible increase of the intake of foods of lower nutritional value, high content of saturated fat and cholesterol, and a decrease of the consumption of meat, fruit, and vegetables. These changes have consequences in terms of body image and interpersonal relationships (Bakker et al., 2018; Park et al., 2014; Ribeiro et al., 2011).
Multipathology and, some pathologies in particular, such as diabetes, hypertension and gastrointestinal diseases sometimes lead to changes in nutrient absorption processes at the level of the intestinal tract; cerebrovascular diseases are often related to changes in swallowing processes such as dysphagia and acute disease. These are other risk factors referred to in the literature (Bakker et al., 2018; Baz & Ardahan, 2019; Boulos et al., 2017; Brabcová et al., 2016; Donini et al., 2013; Melo, 2015; Park et al., 2014; Ribeiro et al., 2011).
Extrinsic risk factors include being single, living alone and being institutionalized (Bakker et al., 2018; Boulos et al., 2017; Donini et al., 2013; Grammatikopoulou et al., 2019; Melo, 2015; Park et al., 2014). Being institutionalized in nursing homes in large cities increases even more the risk of malnutrition due to the social isolation factor (Serrano-Urrea & Garcia-Meseguer, 2013). The older adults that are in nursing homes in small towns/cities seem to have a facilitated maintenance of social interaction/activity (Serrano-Urrea & Garcia-Meseguer, 2013).
The level of education related to the low socioeconomic level influences the individual's nutritional status, as the more educated people find themselves in a more favourable socioeconomic situation (Bakker et al., 2018; Baz & Ardahan, 2019; Boulos et al., 2017; Donini et al., 2013; Grammatikopoulou et al., 2019; Lin et al., 2017; Park et al., 2014).
The reduced number of daily meals (between 2/3) is also a factor that contributes to malnutrition in this population, since the number of minimum meals should be five per day. A lower number means that the individual's nutritional needs are not being met (Baz & Ardahan, 2019; Brabcová et al., 2016).
Polymedication produces side effects at various levels, such as altered taste / smell and reduced salivary secretion with implications for the appetite, decreased absorption for the drug-nutrient interaction, dehydration and constipation (Melo, 2015).
Smoking reduces the function of the taste glands and these, in turn, will decrease the appetite of the older person, being that another factor of relevant risk (Grammatikopoulou et al., 2019; Lin et al., 2017).
Sometimes studies are not clear in what they consider as risk factors and cause (consequence), as they are often used interchangeably, which leads to biased interpretations of the findings that can lead to inaccurate and not very rigorous guidelines/recommendations for practice and political decisions (Moola et. al, 2017). In this study we sought to minimize these biases, seeking to assess a range of risk factors for malnutrition. Still, other studies not included here point to other factors to be taken into account in the population such as low self-perception of health, alcohol consumption or frequent episodes of constipation (Fávaro-Moreira, 2011; O'Keeffe et al., 2019). Within intrinsic/extrinsic risk factors, the literature has highlighted the need for a greater understanding of modifiable risk factors such as lifestyles (smoking, immobility, satisfaction with life). The levels of evidence on the impact of these risk factors are dimensions that deserve further investigation. With an increasingly ageing population, a greater and better understanding of modifiable risk factors, whether intrinsic/extrinsic, will be crucial to the effectiveness of treatment (O'Keeffe et al., 2019).
Conclusions
In this literature review, the main factors that contribute to malnutrition such as age, depression, cognitive deterioration, the presence of multipathologies, and a greater dependence on IADL/AADL were identified, along with the extrinsic factors such as low socioeconomic and educational level and the institutionalization process.
It was noticed that many of the factors are related in a bidirectional way, making it difficult to make predictions between cause and effect. In turn, malnutrition seems to be related to lower functionality and lower quality of life in the older population.
With regard to the usefulness of this systematic review for the clinic, its greatest contribution is given by the identification and systematization of risk factors for malnutrition in the elderly. Health professionals need to be encouraged to carry out periodic assessments of nutritional status, taking into account the risk factors identified as means of screening for possible complications, so that interventions in the context of nutritional promotion can be implemented in a multidimensional and multidisciplinary view.
The training processes of health professionals should explore this population's particularities so that they are trained to provide a type of care that must be increasingly specialized in the needs of the elderly population.
In terms of research, reviews of the produced knowledge are essential tools in terms of planning future research. In this sense, it is believed that this review may be useful for planning objectives and methodologies in the research process within this scope. Cohort studies with several follow-up moments (prospective studies) for the identification and assessment of the impact of these risk factors are necessary, as well as a greater understanding of what is the cause (risk factor) / consequence (effect). It also encourages the development of experimental research in the context of interventions aimed at the various risk factors for malnutrition, especially those with the potential to be modified.
This review, as a secondary investigation process, also has its limitations. The main limitations are the small number of articles included, the lack of evaluation of the methodological quality of these studies (risk of bias) and the heterogeneity between them in terms of context, sample size and methodological processes. Possibly, a broader search, in databases that were not included here, may be a strategy to be adopted in the future in order to minimize most of these limitations

