











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkNailfold capillaroscopy (NC) is a non-invasive imaging technique used in the evaluation of the nailfold capillary network through the intact skin. Its role in the management of connective tissue disorders has been widely described, particularly in systemic sclerosis1. Previous studies have shown its value in the diagnosis and monitoring of dermatomyositis (DM)2. The active involvement of the vascular endothelium in DM induces a complement mediated microangiopathy, with clinical capillary abnormalities in the proximal nail fold (PNF)2.
Although the videocapillaroscope is considered the gold-standard to evaluate nailfold microvascular damage3, this equipment is not widely available in clinical practice, particularly in a dermatology office. Handheld dermatoscope (HD) can partially overcome the lack of videocapillaroscopes3.
The authors report the use of a HD (Dermlite© DL4, × 10 magnification) in a quick and easy evaluation of the PNF capillaries in two patients with DM.
The first patient is a 67-year-old female with DM for 4 years, currently treated with mycophenolate mofetil 2 g/day and prednisone 10 mg/day. Her medical history included inverted and ulcerated Gottron papules, hypomyopathic myositis, and severe interstitial lung disease with pneumomediastinum and cutaneous emphysema, followed within 3 years by breast cancer. Serum myositis autoimmunity panel was positive for anti-SSA2 and anti-MDA5.
At her follow-up visit, skin manifestations of DM as well as lung disease were under control. NC of her digits using a HD revealed enlarged capillaries, microhemorrhages and hyperkeratotic yellow scale in the PNF of some digits (Fig. 1).
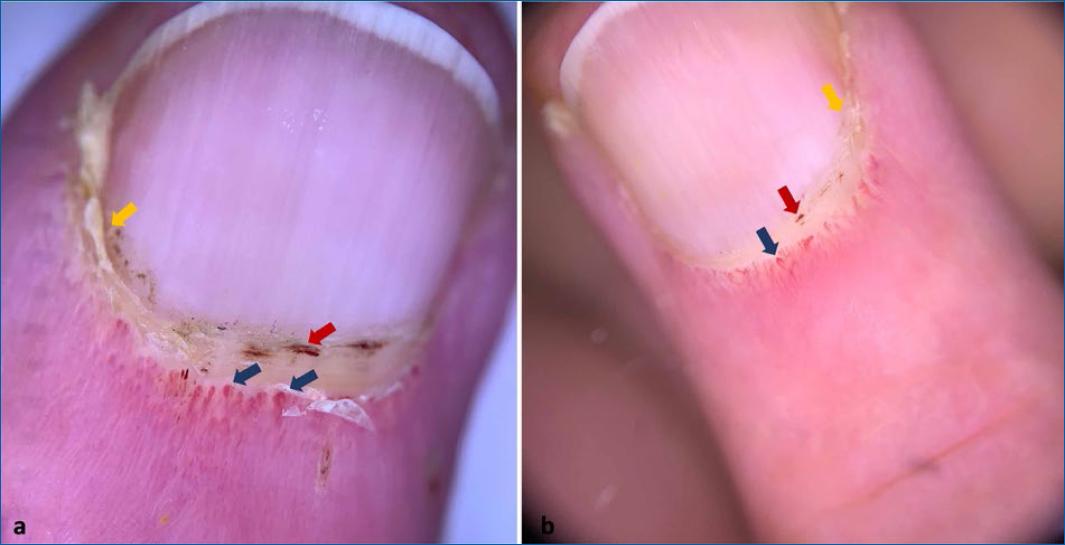
Figure 1 Nailfold capillaroscopy using a handheld dermatoscope in the evaluation of patient 1. Enlarged capillaries (blue arrows–a, b), microhemorrhages (red arrows–a, b) and periungual yellow scale (yellow arrows–a, b) are present. (Dermlite© DL4, x10).
The second patient is a 35-year-old female diagnosed with a 3-year history of DM and breast cancer. No other systemic involvement was present. She was submitted to surgery, chemotherapy and radiotherapy for her cancer. Currently, she is medicated with hydroxychloroquine and topical steroids. Serum work-up detected anti-TIF1-g autoantibodies.
At her follow-up appointment, she presented heliotrope rash, Gottron papules, and an itchy poikiloderma of her upper dorsum. Handheld dermoscopy of the PNF revealed enlarged and ramified capillaries and microhemorrhage (Fig. 2).
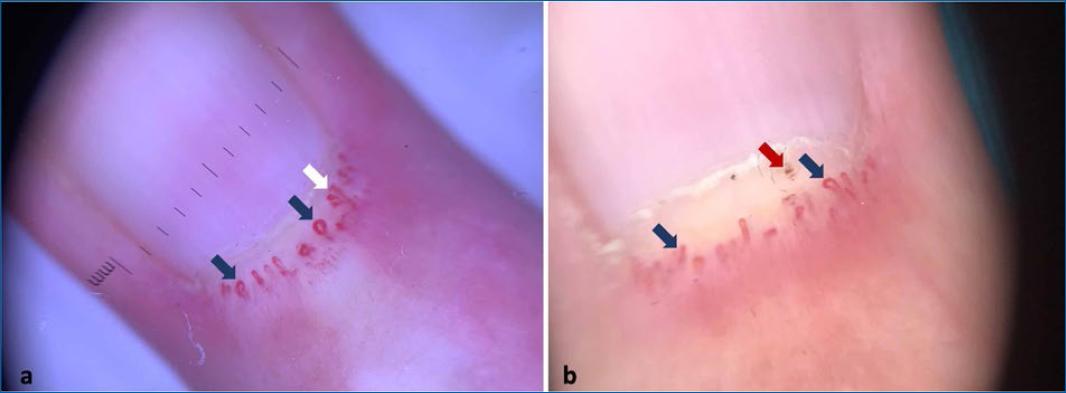
Figure 2 Nailfold capillaroscopy of patient 2 with handheld dermatoscope revealed enlarged capillaries (blue arrows–a, b), ramified capillaries (white arrow–a) and microhemorrhage (red arrow–b). (Dermlite© DL4, x10).
NC is a useful tool for diagnostic purposes in DM. Ramified and giant capillaries, microhemorrhages, vascular disorganization and capillary loss are some of the findings encountered in DM1,2,4. Improvement of the NC abnormalities is expected with the disease stabilization4, although this was not the case in the first patient. Previous studies have suggested NC as a useful tool for assessing muscular and extra-muscular disease in DM4,5. NC abnormalities have been associated with muscle disease activity4, internal malignancies4, skin4 and lung disease5. In fact, a retrospective study with 27 patients with interstitial lung disease (ILD) associated with DM, found that microhemorrhage was significantly higher in patients who died due to ILD5. The authors also found a correlation between the NC findings and the disease activity indicators of DM-ILD. However, the literature is controversial and other studies failed in achieving association between NC abnormalities and muscular/extra-muscular involvement2. Similarly, there isn’t enough evidence that capillaroscopy findings allow distinction between ILD and neoplasia associated DM, or between anti-MDA5 and anti-TIF1-g profiles.
We believe that HD cannot fully replace videocapillaroscopy, since the accuracy for NC abnormalities is lower with the former. However, HD allows a quick screening of the presence of capillary involvement in DM.

