











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
During pregnancy, a woman experiences oral and systemic changes, including behavioral, organic, and physiological alterations at various levels (e.g., endocrine, cardiovascular, respiratory, immunological, and neurological).1-3 Some of these changes can lead to a greater susceptibility to specific oral pathologies, both in terms of soft and hard tissues.1,4-6 However, inadequate attention to oral health during pregnancy is commonly reported.
Poor attention to oral health often leaves pregnant women susceptible to oral problems, such as pain, and increased levels of anxiety largely related to adverse pregnancy outcomes.2,7-9
Moreover, cumulative evidence has associated periodontal diseases in pregnant women with adverse pregnancy outcomes, including preeclampsia, gestational diabetes, preterm birth, and low birth weight.10-13 Research has further shown that the mother’s oral condition and behaviors significantly influence the offspring’s oral health outcomes, particularly the risk of experiencing early childhood caries (ECC).10,15-16
Considering the inherent oral implications of pregnancy and the potential systemic consequences, timely monitoring and early intervention are extremely important. Therefore, monitoring oral health in pregnant women should be an integral part of the approach to their general healthcare.4,5,7,17-19
During the prenatal period, pregnant women show greater interest and receptivity in acquiring information and changing their health habits and practices.4,5 Oral health education covering the prevention of oral diseases and demonstrating correct practices can then be provided. In addition, periodic consultations should be encouraged, as they bring importante benefits for both pregnant women and their children.4,16,18,20,21
Previous studies have found evidence of knowledge gaps and misconceptions among expectant mothers concerning: oral hygiene habits, the incidence of various oral pathologies, dental treatment, and poor oral health and its impact on the course of pregnancy and ECC.17,18,21-27 Multiple barriers to accessing oral healthcare during pregnancy have also been identified in several countries.8,9To our knowledge, available data among pregnant women in Portugal is limited, as the few published
studies involved small sample sizes and did not fully record the participants’ knowledge of the impact of maternal oral health and behavior on children’s oral health.28,29Accordingly, the present study aims to assess the effect of maternal knowledge and practices on prenatal and infant oral health, with a survey of pregnant women followed in two Portuguese public health institutions.
Material and methods
This cross-sectional survey was performed using a convenience sample of pregnant women attending pre-scheduled consultations for routine prenatal follow-up at a public maternity practice and a family health facility in Coimbra, Central Portugal. A total of 120 pregnant women were eligible to enroll in the study: 82 from the public maternity system, 19 from the family health facility, and 19 from individual contacts of the researchers. All women agreed to participate in this study. Data collection occurred over two consecutive months on randomly selected days.
The research fully complied with the ethical requirements of the 1964 Helsinki declaration and its later amendments. Required authorizations were obtained from both institutions prior to commencing the study. After giving written informed consent, each participant was asked to complete a self-reported questionnaire. Exclusion criteria included non-Portuguese speakers and unwillingness to participate.
The questionnaire, based on previously published surveys,22,23,25 consisted of 29 closed-answer questions covering sociodemographic information, oral health knowledge and practices in pregnancy, and the pregnant woman’s knowledge of oral health in children.
The results of the questionnaires were entered into Microsoft Excel® 2011 for subsequent statistical treatment using IBM SPSS Statistics21. A descriptive analysis was performed, and the independence of the variables was checked with the chisquare test (χ2) under a 95% confidence interval (p<0.05).
Results
The sociodemographic profile of the sample is shown in Table 1. Approximately half of the respondents (52.5%) were aged between 31 and 35 years old, 71.7% had attended higher education, 64.0% were married, and 71.7% lived in urban areas (Table 1). This was the first pregnancy of most women, and 52.5% were in the last trimester of pregnancy (Table 1).

Concerning attitudes and behaviors of pregnant women regarding their oral health, 68.9% reported brushing twice a day, and 36.4% said they did not use dental floss as an additional measure (Table 2). As a group, pregnant women below 25 years stood out due to their low use of dental floss, with a statistically significant association (p=0.004; χ2=14.329) between using dental floss and age (Table 2).
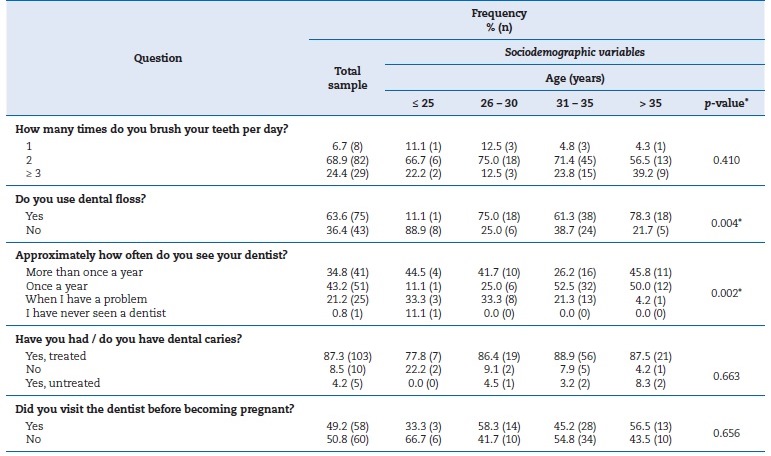
When asked about the frequency of dental appointments and prior history of dental caries, 43.2% of respondents confirmed they regularly attended annual consultations, and most (87.3%) said they had previously had caries lesions treated (Table 2). About 60.8% of the respondents rated their current oral health status as “Good”, while 31.7% rated it as “Acceptable” and 7.5% as “Excellent”. However, only 49.2% of the pregnant women had undergone dental appointments before their current pregnancy (Table 2).
Regarding the oral health-related knowledge of pregnant women, most participants (83.3%) responded positively when asked about the possibility/need to undergo dental treatment during pregnancy (Table 3). Nonetheless, over half of the respondentes (59.2%) agreed that pregnancy could be harmful to their oral health, with a statistically significant association to their age groups (p=0.010; χ2=17.165) and level of education (p=0.037; χ2=15.965) (Table 3). When asked, “Do you think that caries is a communicable disease?”, 69.2% of women gave a negative response and 20.8% did not have an opinion (Table 3). Similarly, 58.3% stated they were unaware that gingivitis or periodontitis could contribute to premature birth and low birth weight (Table 3).

Most pregnant women showed a lack of knowledge of the importance of diet in oral health, with 71.8% stating they did not know the importance of diet to their oral health. A statistically significant association was found between the response to this question and the frequency of regular dental appointments (p=0.035; χ2=14.328) (Table 3).
Regarding ECC, 43.3% of participants reported they were unaware of the existence of this disease. A statistically significant association was found between this variable and both the level of education (p=0.034; χ2=14.283) and the environment where they lived (rural/urban) (p=0.015; χ2=8.501); the latter association was also found when considering only women in first pregnancies (p=0.027; χ2=7.340) (Table 4). When asked about the relationship between caries and nocturnal breastfeeding, 37.5% of respondents stated they did not know whether they were related and 46.7% thought they were unrelated (Table 4).
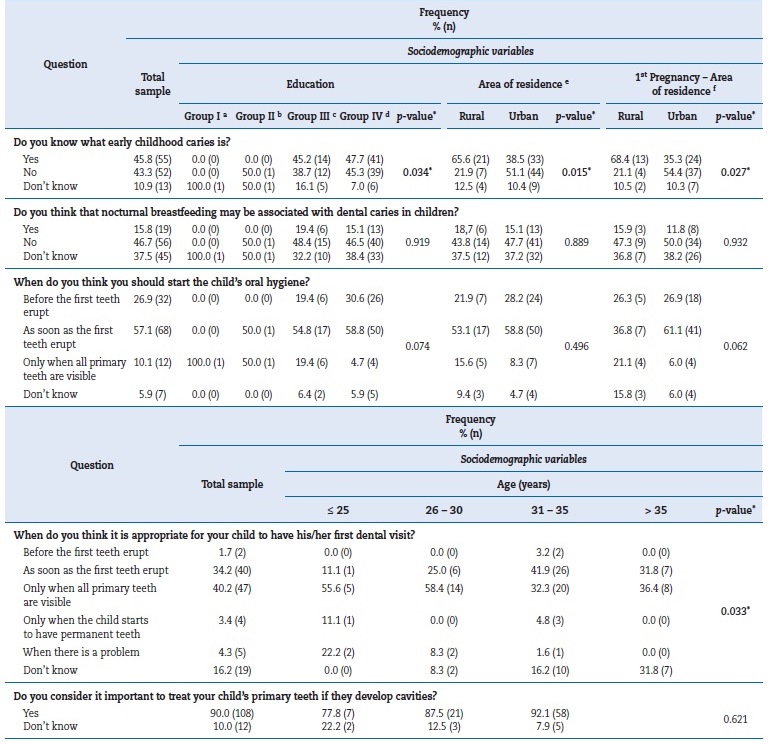
The majority of participants (84.0%) considered that the appropriate time to start oral hygiene is before or as soon as the first teeth erupt (Table 4). However, only 35.9% of expectant mothers considered the first dental appointment should occur before or as soon as the child’s first teeth erupt. Some participants stated the child’s first dental visit should occur only when all primary teeth are visible (40.2%), when there is a problem (4.3%), or when the child has permanent teeth (3.4%) (Table 4). A statistically significant association was found between this variable and age (p=0.033; χ2=27.287). Most respondents (90.0%) recognized the importance of treating injuries to primary teeth (Table 4).
Discussion
The present study aimed to assess the effect of maternal knowledge and practices on prenatal and infant oral health, with a survey of pregnant women followed in two Portuguese public health institutions.
From the results, most pregnant women reported toothbrushing twice daily. Previous studies have reported a correlation between this practice and higher levels of education,7,23,25,30 and indeed, most of this study’s sample reported having attended higher education (71.7%). However, 36.4% of participants said they did not floss, which is consistent with findings from a previous report among expectant women in Portugal.29 Most notably for this study, those under 25 years old were more likely not to use floss, thus highlighting the importance of hygienic instruction and motivation.
Although only a minority reported never having gone to a dental consultation, half the respondents had not visited the dentist before becoming pregnant. The latter finding is, unfortunately, in line with previously reported practices.8,9,29This negligence happens despite the known established effect of prenatal oral health care on preventing adverse birth outcomes and ECC onset.11,16 Nonetheless, most participants stated they would undergo dental treatment during pregnancy if needed. While these results may reveal that the women surveyed were aware that dental treatment during pregnancy was safe, another possible explanation is the misconception, supported by over half of the participants, that pregnancy can be potentially harmful to their oral health. This result is consistente with previous findings from another cohort followed in the same public maternity practice, where the persistence of myths about the effects of pregnancy on oral health was also reported, particularly an increased tendency for dental demineralization and tooth loss.28
Additional knowledge gaps were identified, as more than half of the pregnant women were unaware that gingivitis or periodontitis could contribute to premature birth and low birth weight, corroborating the findings of previous international surveys.17,31 Insufficient knowledge regarding the importance of diet in oral health was found among most respondents, despite dietary factors being fundamental to the etiology of multiple oral pathologies, both for pregnant women and children.21,32,33
Lamentably, it was evident that a high proportion of the cohort was not familiar with ECC. Similar to earlier reports, most participants in this study also said that caries was not communicable or did not know whether it was. This finding possibly reveals an unawareness that early acquisition of Mutans Streptococc is a key risk factor for developing ECC.14-16,29,34,35 The fact that mother-to-child (or caregiver-to-child) transmission constitutes the major pathway for Mutans Streptococci initial acquisition underlines the importance of education and prenatal oral health care in reducing maternal carriage of Mutans Streptococci and limiting saliva-sharing activities, as highlighted by recent studies.14-16,33
A substantial number of pregnant women stated that nocturnal breastfeeding was not associated with the etiology of ECC. In fact, although multiple studies have explored the potential impact of prolonged and ad libitum breastfeeding on ECC’s development, recent evidence from a systematic review suggests that breastfeeding does not increase ECC risk.21,36
Regarding perinatal oral health care, most pregnant women recognized the importance of treating primary teeth and stated their intention to establish toothbrushing habits before or as soon as the first teeth erupted, a finding in line with those of Ferreira et al.29 Nonetheless, while one-third of the sample intended that their child first visited the dentist as soon as teeth erupted, a large proportion of participants reported an intention to visit the dentist only when all of the child’s primary teeth were present. Another concerning finding is that a non-negligible share of participants stated they did not know when the first dental appointment should occur.
Such lack of knowledge reduces the likelihood of establishing a dental home during the child’s first year of life, a crucial recommendation for establishing oral health preventive and/or curative strategies.4,33,37,38
This research presented some limitations. Firstly, there are known possible drawbacks of questionnaire-based studies: nonresponses, misconceptions, and socially desirable answers.
Another limitation is related to the nature of the cohort, particularly the asymmetric distribution of sociodemographic characteristics. Despite recognizing that the present sample cannot be considered representative of all pregnant women in Portugal, to the best of our knowledge, this study involved a considerably larger sample than the few published surveys among Portuguese cohorts.28,29
Even though our results generally reflect those found in the international literature,7,17,19,21-27,30,39such a comprehensive characterization of oral health-related knowledge and the practices of expectant mothers has not been reported for Portuguese cohorts. This work enabled the identification of importante gaps and illustrated the urgent need for prenatal education and promotion of oral health in Portugal.
Conclusions
Most pregnant women taking part in this study believed pregnancy could be harmful to their oral condition, and a significant proportion did not seek prenatal oral health care. Surveyed women also lacked knowledge of the potential impact of their periodontal status on gestation and were unaware of the existence of ECC and the need for its prevention, particularly regarding concepts such as vertical transmission and the establishment of a dental home. This study population showed a clear demand for the implementation of educational programs aimed at increasing awareness and understanding on these matters.

