











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Case Presentation
A 54-year-old man with left elbow pain 2 months. Denies recent trauma and diseases, referring to being a handyman. He reports fracture of the radial head performing replacement with silicone prosthesis nine years ago, without complications since then. Physical examination shows elbow edema with reduced strength in the affected upper limb, without signals of numbness. No limitation of movement.
The computed tomography scan demonstrates a fracture of the neck of the silicone prosthesis of the radius head, with slight lateral displacement of the prosthesis head), irregularity of the capitellum, and of the radial notch (Figure 1). The patient was referred to the orthopedics department for scheduling surgery.
Discussion
The radial head is an important secondary stabilizer of the elbow and can bear up to 60% of the load transmitted from the forearm.1,2 Replacement of the radial head is advised in cases in which the extent of ligamentous injury calls for this secondary stabilizing function and it is not possible to reconstruct the radial head.1
The goals of treating radial head fractures are to restore stability, preserve motion, and maintain the length of the radius.2 If preservation of the head is not possible, prosthetic replacement has been advocated to preserve the radiocapitellar articulation.2 Many radial head implant materials are possible, including metal, pyrolytic carbon (pyrocarbon), and silicone.2,3 Silicone was introduced by Swanson in 1969.3
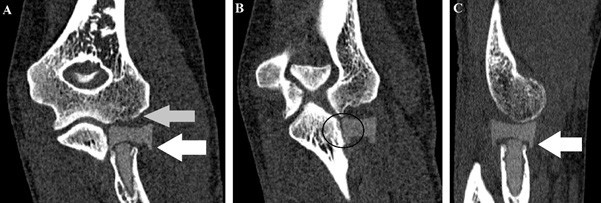
Figure 1: CT Scan of the left elbow in coronal section in A and B, and in sagittal section in C, demonstrating fracture of the neck of the silicone prosthesis with slight lateral displacement (white arrow), irregularity of the capitellum (grey arrow) and of the radial notch (black circle).
A head and neck segment that is made of silicone is embedded after radial head resection.3 Silicone hemiarthroplasty is barely executed because of a huge percentage of loosening, fracture, and silicone synovitis.3 Nevertheless, radiologists, sometimes, encounter patients who received this sort of implant during the 1970s and 1980s.3
The inability of a silicone radial head to resist compressive loads or valgus stress is evidence that the implant does not restore normal radiocapitellar load transmission, which is believed to be imperative for normal elbow function.4 At radiography, it is essential the evaluation for fracture of the silicone and silicone synovitis, which are seen as periprosthetic lucencies and soft-tissue swelling.3 The fractures of silicone radial head implant arthroplasty include prosthetic fracture at the head, stem-head junction, or stem.4
After implant failure, bone resorption has been reported around silicone finger-joint implants and wear particles have been implicated as causing synovitis and subchondral bone cysts.5 An irregular capitellum may cause fraying of the implant surface and release of particulate silicone debris because of shear and abrasive wear, evidenced clinically by the high incidence of squeaking sounds with forearm rotation.4 Silicone prosthesis turned out to be biologically and biomechanically insufficient.5

