










Servicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versión impresa ISSN 2341-4545
GE Port J Gastroenterol vol.24 no.6 Lisboa dic. 2017
https://doi.org/10.1159/000477738
ENDOSCOPIC SNAPSHOT
Percutaneous Transhepatic Cholangiography Rendez-Vous Procedure to Reach the Duodenum for Enteroscopy-Assisted Endoscopic Retrograde Cholangiopancreatography in Surgically Altered Anatomy
Colangiopancreatografia Retrógrada Endoscópica com Enteroscópio com Técnica de Rendez-Vous com Colangiografia Percutânea Trans-Hepática para Alcançar o Duodeno em Doente com Anatomia Cirurgicamente Modificada
Ana Pontea, Rolando Pinhoa, Luísa Proençaa, Joana Silvaa, Jaime Rodriguesa, Mafalda Sousaa, Tiago Pereirab, João Carvalhoa
Departments of aGastroenterology and bRadiology, Centro Hospitalar de Vila Nova de Gaia Espinho,Vila Nova de Gaia, Portugal
* Corresponding author.
Keywords: Endoscopic retrograde cholangiopancreatography,·Single-balloon enteroscopy, Percutaneous transhepatic cholangiography, Choledocholithiasis
Palavras-Chave: Colangiopancreatografia retrógrada endoscópica,·Enteroscopia assistida por monobalão, Colangiografia percutânea trans-hepática, Litíase biliar
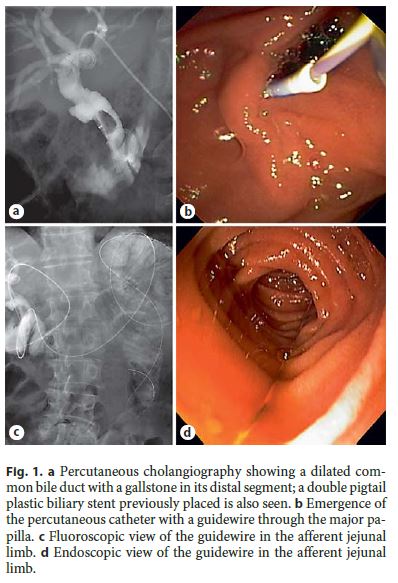
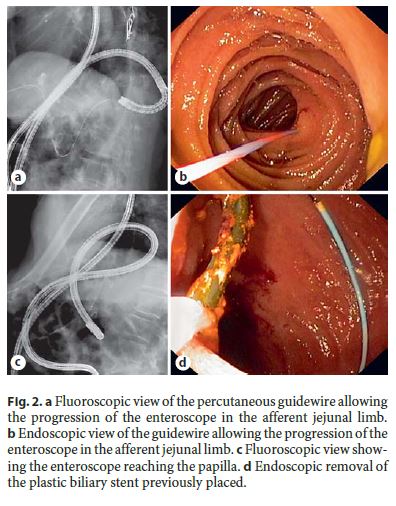
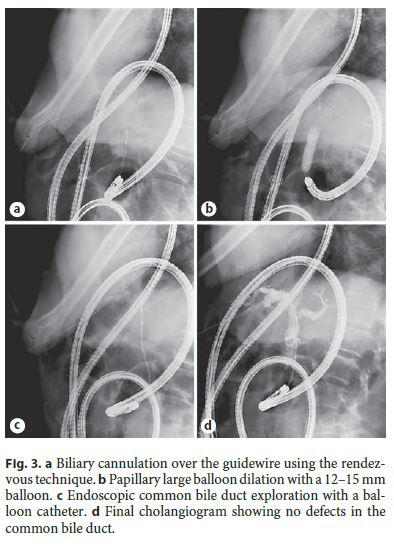
The present case reports a 78-year-old male with a history of total gastrectomy with Roux-en-Y anastomosis and splenectomy for gastric cancer in 2007 and cholecystectomy in 2014 for cholelithiasis. The patient presented with a 1-week history of abdominal pain, fever, and vomiting. Laboratory tests revealed leukocytosis (17,290 . 10 3 /μL [normal range: 3.8–10.6]) and elevated total bilirubin (3.75 mg/dL [0.1–1.1]), conjugated bilirubin (2.89 mg/dL [0.1–0.3]), aspartate aminotransferase (364 mg/dL [4–33]), and alanine aminotransferase (198 mg/dL [4–50]). Abdominal ultrasound revealed a 13-mm gallstone in the common bile duct, resulting in its dilation up to 15 mm. After conservative management for acute cholangitis, the patient was referred for singleballoon enteroscopy (SBE)-assisted endoscopic retrograde cholangiopancreatography (ERCP). During SBEERCP (with carbon dioxide insufflation), since only limited sphincterotomy could be performed due to limitations in the orientation of the available sphincterotome (CCPT-25ME; Cook Medical Inc., Bloomington, MN, USA), large balloon dilation (LBD) up to 12 mm was performed. Despite LBD, stone extraction was impossible, and a 3-cm long, 7Fr double pigtail plastic biliary stent was thus placed. A second SBE-ERCP was performed 3 months later to complete the procedure, but the papilla could not be reached due to fixed angulations that caused recurrent looping of the enteroscope, despite changes in position and abdominal compressions. Therefore, a third SBE-ERCP using the rendez-vous technique was planned to reach the papilla. A percutaneous transhepatic cholangiography was performed to insert a 0.035 600-cm guidewire (METII-35–600E; Wilson-Cook Medical Inc., Limerick, Ireland) in antegrade direction (Fig. 1a) through the major papilla (Fig. 1b) into the afferent limb (Fig. 1c). The SBE was advanced to the afferent limb (Fig. 1d) where the guidewire was grasped with a polypectomy snare. Maintaining external traction in the guidewire (Fig. 2a, b), progression of the enteroscope to the papilla was achieved (Fig. 2c) where the previously placed biliary stent was identified. The biliary stent was removed (Fig. 2d), and biliary cannulation was performed over the guidewire using the rendezvous technique (Fig. 3a). LBD with a 12–15 mm balloon was subsequently performed (Fig. 3b), followed by endoscopic common bile duct exploration with a balloon catheter resulting in extrusion of the stone and biliary sludge (Fig. 3c, d). The patient was discharged 1 day after the procedure and remains asymptomatic after 11 months of follow-up.
ERCP in patients with surgically altered upper gastrointestinal anatomy such as total gastrectomy is challenging [1–3]. SBE-ERCP may overcome those limitations, as the enteroscope allows deep insertion into the small bowel and access to the papilla and the biliary tract [1, 3, 4]. Nevertheless, current evidence demonstrates that the enteroscopy success rate (defined as success in reaching the papilla and/or biliary anastomosis) of SBE-ERCP among different studies ranges from 55 to 100% [4] . The common reasons for the lack of enteroscopy success include failure to identify the afferent limb of the Roux-en-Y anastomosis, sharp small bowel angulations, adhesions, recurrent looping, and anastomotic stenoses [4]. Some techniques may be used to identify the afferent limb, such as the injection of Indigo carmine or CO 2 , or to reach the papilla, such as abdominal compressions or changes in position. The rendez-vous technique with percutaneous transhepatic cholangiography [5] is useful when reaching the papilla is unsuccessful despite the use of the previously mentioned techniques, as highlighted in this case.
References
1 Pinho R, Proenca L, Alberto L, Carvalho J, Pinto-Pais T, Fernandes C, et al: Biliary selfexpandable metallic stent using single balloon enteroscopy assisted ERCP – overcoming limitations of current accessories. Rev Esp Enferm Dig 2013; 105:561–564. [ Links ]
2 Yamauchi H, Kida M, Imaizumi H, Okuwaki K, Miyazawa S, Iwai T, et al: Innovations and techniques for balloon-enteroscope-assisted endoscopic retrograde cholangiopancreatography in patients with altered gastrointestinal anatomy. World J Gastroenterol 2015; 1:6460–6469. [ Links ]
3 Pinto-Pais T, Pinho R, Proenca L, Fernandes C, Ribeiro I, Pereira T, et al: Single-balloon enteroscopy assisted endoscopic retrograde cholangiopancreatography with the rendezvoustechnique. GE Port J Gastroenterol 2015;22:39–41. [ Links ]
4 Inamdar S, Slattery E, Sejpal DV, Miller LS, Pleskow DK, Berzin TM, et al: Systematic review and meta-analysis of single-balloon enteroscopy-assisted ERCP in patients with surgically altered GI anatomy. Gastrointest Endosc 2015;82: 9–19. [ Links ]
5 Pinho R: The vanishing frontiers of therapeutic enteroscopy. GE Port J Gastroenterol 2015;22:133–134. [ Links ]
Statement of Ethics
This case required informed consent but did not require review/approval by the appropriate ethics committee.
Disclosure Statement
The authors have no conflicts of interest to declare.
* Corresponding author.
Dr. Ana Ponte
Department of Gastroenterology, Centro Hospitalar de Vila Nova de Gaia Espinho, Rua Conceicao Fernandes
PT–4434-502 Vila Nova Gaia (Portugal)
E-Mail ana.ilponte@gmail.com
Received: December 5, 2016; Accepted after revision: April 13, 2017

