











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkA 66-year-old female patient presented for screening colonoscopy after an incomplete office-based procedure due to failed sigmoid passage. Medical history included hysterectomy with adnexectomy and appendectomy. Apart from cecal angiodysplasias, a tenacious mucus lake was detected at the appendix base (“cecal mucus sign”) [1, 2] (Fig. 1a). After extensive washings, at first, no clear-cut mucosal abnormality was identified by white light and image-enhanced endoscopy (Fig. 1b, c). Only after manipulation by a standard biopsy forceps, a submerged lesion was unmasked, pathologically confirmed as a sessile serrated adenoma/polyp (SSA/P) without dysplasia (Fig. 1d). In consideration of her significant surgical history, nota bene including appendectomy, and significant obesity (BMI 43.0 kg/m2), we abstained from up-front surgery for this benign colorectal lesion, and the patient consented to undergo endoscopic resection [3]. However, the intended device-assisted endoscopic full-thickness resection (EFTR) could not be performed due to lack of passage through the sharply angulated sigmoid by the full-thickness resection device (FTRD) test cap (FTRD prOVE Cap, Ovesco, Germany) [4]. Beyond the previously detected small sessile lesion, the full lesion extent was, at the time, visualized after ineffective submucosal indigo carmine injection related to exuberant postsurgical fibrosis and acetic acid spraying, albeit as yet with lowlevel evidence, highlighting the serrated lesion and its borders [5, 6]. The appendix rest was, in addition, distended by underwater endoscopy, revealing a carpet-like involvement with a diffusely velvety appearance (Fig. 1e). Albeit post-piecemeal endoscopic mucosal resection (pEMR) surveillance has been scheduled in 9 months and is, thus, still pending, presumably complete pEMR was achieved by cold snare resection of sessile parts, and na uncomplicated (standard) cap-assisted aspiration mucosectomy of the remaining appendix (Fig. 1f). Visualization of the resection bed excluded deep mural injury and/ or bleeding-prone vessels, thus clip-closure of the defect was not warranted, and the patient took an uncomplicated clinical course. Notwithstanding that recent data indicate feasibility of simple EMR in appendiceal lesions involving < 50 % of the circumference with an identifiable proximal extension, the presented clinical report is unique in terms of status post-appendectomy as well as a carpetlike, utterly flat extension of an estimated 15-mm serrated lesion occupying the whole appendix rest [7].
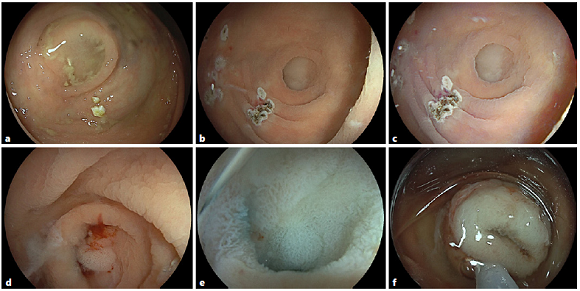
Fig. 1 a A “cecal mucus sign” was identified during screening colonoscopy. b, c After extensive washings, no clear-cut mucosal abnormality was identified by white light and image-enhanced endoscopy - note argon plasma coagulation (APC) sites due to cecal angiodysplasias. d Only after forceps manipulation, a submerged lesion was unmasked, pathologically confirmed as a sessile serrated adenoma/polyp (SSA/P) without dysplasia. e Beyond previously detected small sessile parts, the full lesion extent was visualized after acetic acid spraying and underwater endoscopy, revealing a carpet-like involvement with a diffusely velvety appearance. f Endoscopic piecemeal resection was achieved by cold snare resection and cap-assisted aspiration mucosectomy.

