Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
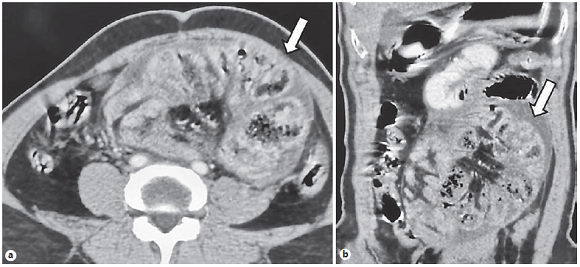
PermalinkA 58-year-old man presented with complaints of abdominal pain and bilious vomiting for 2 days. Twenty days before, he had undergone exploratory laparotomy with adhesiolysis, segmental ileal resection, and end ileostomy for acute intestinal obstruction and ileal gangrene. Contrast-enhanced computed tomography (CECT) showed clumping of ileal loops surrounded by a thick membrane (“cauliflower sign”) (Fig. 1) consistent with encapsulating peritoneal sclerosis (EPS). Clumping of dilated small bowel loops in a narrow base surrounded by a thick membrane seen on CT in patients with EPS or the abdominal cocoon is called the “cauliflower sign” [1, 2]. EPS is characterized by the partial or total encasement of the small bowel by a fibro-collagenous membrane. It can be idiopathic or due to abdominal tuberculosis, chronic peritoneal dialysis, peritoneovenous shunts, sarcoidosis, use of drugs, such as propranolol, and abdominal surgeries [2]. All these conditions cause peritoneal irritation and inflammation, which leads to fibrosis. The “cauliflower sign” is also seen on ultrasound and barium studies [2, 3]. Differential diagnoses include congenital peritoneal encapsulation, peritoneal carcinomatosis, and internal hernias [2]. Though traditionally managed surgically with dissection of the abdominal cocoon and extensive interbowel adhesiolysis, conservative medical treatment with renin-angiotensin-aldosterone system blockers, immunosuppressants, and tamoxifen have been currently used with variable success rates [2]. EPS in this particular case is probably related to the major abdominal surgery performed 20 days before. The patient underwent surgery for simple removal of the membrane and lysis of the adhesions.