











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkA 67-year-old female patient presented for sigmoidoscopy 12 months after complex endoscopic resection in the rectum. This included piecemeal endoscopic mucosal resection (peripheral parts) coupled with central device-assisted endoscopic full-thickness resection (EFTR; Full-Thickness Resection Device; Ovesco, Tübingen, Germany) for a large supra-anal EMR recurrence with marked fibrosis. Pathology confirmed low-grade adenoma at the time. At the recent endoscopy, an estimated 10-mm, nodular lesion emerged within the otherwise unremarkable resection site with exuberant fibrosis (Fig. 1a). Consistent with the initial endoscopic impression, further assessment using linked color imaging (Fig. 1b) and blue laser imaging did not suggest neoplastic surface and/or irregular vessel pattern (Fig. 1c). With an aim to achieve a distinct tissue diagnosis of this presumed clip artifact, the lesion was resected en bloc by conventional mucosectomy. Pathology indicated presence of a nodular proliferation of eosinophilic spindle-shaped cells devoid of nuclear atypia (Fig. 1d: HE. ×1.6; Fig. 1e: HE. ×5). Ancillary immunohistochemistry including CD34, CD117, DOG-1 (discovered in gastrointestinal stromal tumor-1), and smooth muscle actin (SMA) confirmed SMA to be exclusively expressed within this leiomyoma-like mesenchymal proliferative lesion (Fig. 1f: SMA, ×5).
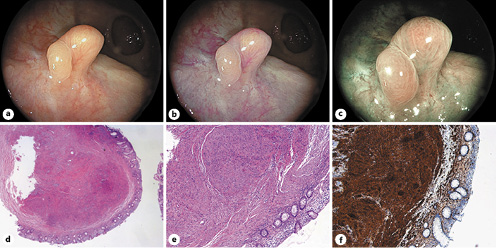
Fig. 1: a An estimated 10-mm, nodular lesion within the otherwise unremarkable resection site with exuberant tissue fibrosis. b, c Image-enhanced endoscopy using linked color imaging and blue laser imaging without evidence of neoplastic surface and/or vessel pattern alterations. d, e Pathology indicates a nodular proliferation of eosinophilic spindle-shaped cells without nuclear atypia (HE, ×1.6 and ×5, respectively). f Immunohistochemistry staining for SMA indicates high lesional expression, while immunohistochemistry for CD34, CD117, DOG-1 (discovered in gastrointestinal stromal tumor-1) proved unremarkable (SMA, ×5).
Device-assisted EFTR has gained much momentum in recent years for the endoscopic resection of selected colorectal lesions [1]. However, the full spectrum of EFTR-related, novel clip artifacts, reflective of transmural tissue capture, is still unfolding, with which endoscopists should become acquainted to avoid undue procedures such as re-do EFTR and/or surgery [2-4].

