











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
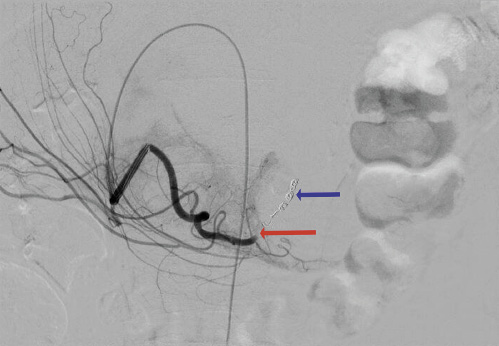
PermalinkA 58-year-old male with dysphagia due to a hypopharyngeal squamous cell carcinoma underwent a percutaneous endoscopic gastrostomy (PEG) tube placement by the pull technique into the anterior gastric wall between the corpus and antrum without immediate complications (Fig. 1). Two and three weeks later, he was admitted with hypotension and melena, with no changes in the gastrostomy site and hemoglobin of 5.1 and 6.0 g/dL (baseline value: 8.5), respectively. Tumor friability bleeding was assumed; the patient received red blood cells, started an oral antifibrinolytic agent, and was discharged. A month after the procedure, he was readmitted with similar symptoms, a new drop of 3 g/dL in hemoglobin, and a 10-mm palpable mass under the external PEG tube. An abdominal computed tomography revealed a 17 × 7 × 10 mm pseudoaneurysm arising from the gastroduodenal artery (Fig. 2). An angiography showed contrast extravasation from the gastroduodenal artery (Fig. 3) and embolization with coils (Fig. 4) was successfully performed. Three months after the procedure the patient remains asymptomatic.

Fig. 1: Endoscopic image showing the site of percutaneous endoscopic gastrostomy placement in the anterior gastric wall between corpus and antrum.
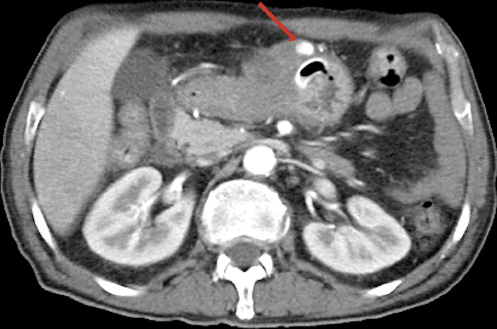
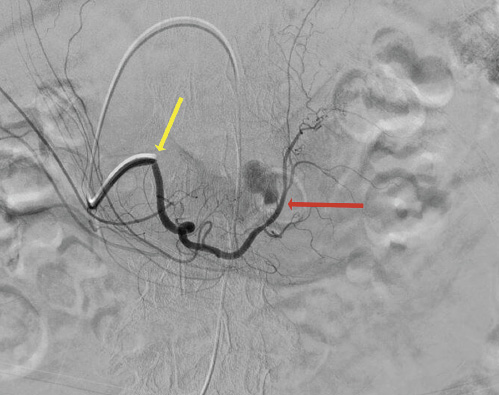
Fig. 3: Angiography revealing contrast extravasation (red arrow) from the gastroduodenal artery (yellow arrow).
Hemorrhage following gastrostomy tube placement occurs in 0.6-1.2% of cases. Bleeding originates mostly from the gastrostomy tract or from gastric ulceration [1]. Less common causes of bleeding include gastric artery perforation, superior mesenteric artery perforation, retroperitoneal hemorrhage, aortic perforation, abdominal wall pseudoaneurysm, and gastric wall and rectus sheath hematomas. PEG site hemorrhage caused by a pseudo aneurysm is exceedingly rare with only few cases reported in the literature. They resulted from direct arterial injury during the PEG tube placement. Given that the PEG tube placement typically involves the anterior wall of the stomach, the possibility of an arterial puncturing seems low. However, the rotated structure of the stomach and/or an angiectopia can explain an inadvertent arterial puncture. In all described cases, patients underwent PEG tube placement with the “pull” technique and presented few weeks later with recurrent episodes of upper gastrointestinal bleeding. Computed tomography angiography and Doppler ultrasound contributed to establish the definitive diagnosis. In most cases, the treatment involved interventional radiology with angiographic embolization or surgery [2, 3]. Percutaneous thrombin injection was used as an alternative to surgical or endovascular therapy in a patient with kidney injury and obesity [4].
PEG site hemorrhage caused by a pseudoaneurysm is a differential diagnosis to keep in mind in a patient with recurrent upper gastrointestinal bleeding after PEG tube placement. The diagnosis of this potentially fatal complication implies a high suspicion index due to its nonspecific presentation and rarity. Angiographic embolization constitutes an effective therapy.

