











 (pdf)
(pdf)




 SciELO
SciELO  SciELO
SciELO 
 Permalink
Permalink
A 44-year-old female patient was subjected to total colonoscopy that revealed a 15 mm bulge in the cecum, covered by normal mucosa, compatible with subepithelial lesion, of hard consistency and no pillow sign (Fig. 1a). The lesion was evaluated by ultrasonography with mini-probe (Fig. 1b), which confirmed the presence of a sub-epithelial nodular hypoechoic lesion although it was not possible to safely distinguish between the second and third ultrasonographic wall layers.
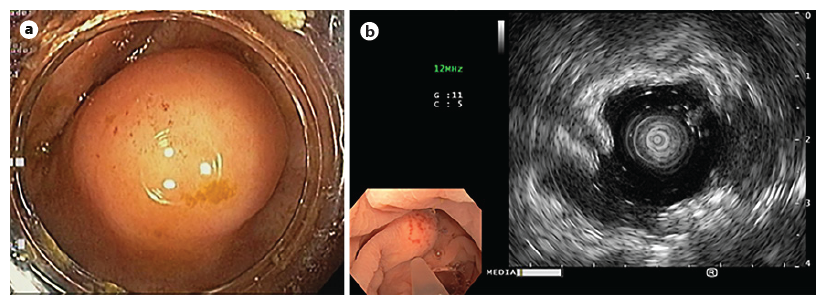
Fig. 1. Endoscopic findings. a In the cecum, a 15 mm bulge with normal mucosa was observed. b Ultrasonography - a subepithelial nodular lesion was confirmed, although it was not possible to safely distinguish between the second and third ultrasonographic wall layers.
Endoscopic submucosal dissection (ESD) was pro-posed. The endoscopist had extensive experience in colorectal ESD. A glycerol solution with indigo carmine and adrenaline (1:50,000) was injected (Fig. 2a). Mucosal incision was performed (Fig. 2b), followed by submucosal endoscopic dissection using DualKnife JTM (Olympus, Tokyo, Japan) and IT Knife nanoTM (Olympus, Tokyo, Japan), with dry-cut current effect 2.5 and swift coagulation current effect 3 achieving total excision of the lesion at the end of the procedure (Fig. 2c-e). The scar was closed with Resolution 360TM ULTRA clips (Boston Scientific, Boston, USA) (Fig. 2f, g). The lesion was retrieved en bloc (Fig. 2h). No adverse events were observed.
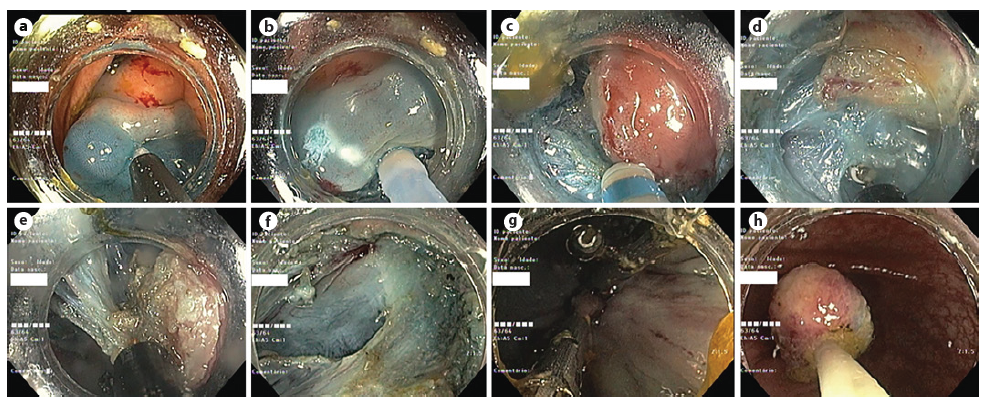
Fig. 2. Endoscopic submucosal dissection. a Submucosal injection. b Mucosal incision. c-e Submucosal dissection. f Dissection scar. g The scar was closed with clips. h En bloc lesion retrieval.
Histological evaluation revealed a solid neoplasia of the submucosa consisting of epithelioid cells of vast granular citoplasma, centered by small, round, uniform nuclei (Fig. 3a, b). These cells were positive for S100 and inhibin - granular cell tumor (GCT) (Fig. 3c, d). The lesion was limited to the submucosa and was covered by normal colonic mucosa. The excision margins were free. A surveillance colonoscopy at 12 months is currently scheduled.
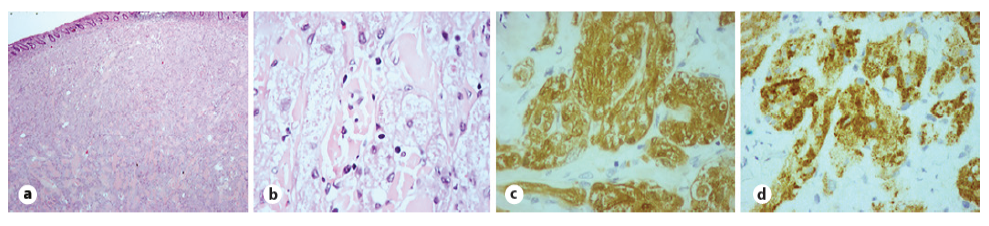
Fig. 3 Histological evaluation. a Submucosal expansion by epithelioid cells, covered by normal colonic mucosa (×20 magnification). b These cells have vast granular citoplasma, centered by small, round, uniform nuclei (×100 magnification). c, d Immunohistochemistry showing positivity for S100 (c) and inhibin (d) (×400 magnification).
The authors present a case of a subepithelial lesion in the cecum evaluated by miniprobe ultrasonography and removed en bloc by ESD. GCT’s are a rare entity, whose pathological behavior is not fully understood, and are most frequently found incidentally. Granular cells have neuronal origin, and Schwann cells are precursors [1, 2].
The cases reported in the literature suggest a generally benign behavior but <2% have shown potential for malignancy, which is suggested by endoscopic features of ulceration or size >40 mm [3]. Histological proposed criteria for malignancy are the following: high number of mitosis, big nuclei, signs of lymphovascular invasion; evidence of metastization being the sole definitive criteria [2]. A case of local recurrence due to incomplete resection was reported [3]. ESD in the colon is a safe, technically demanding procedure that allows an en bloc resection and avoids surgery in the absence of features of malignancy. Endoscopic fullthickness resection using a full-thickness resection device is an alternative and developing method, with current evidence apparently showing a similar safety profile albeit with a lower complete resection rate [4]. To the best of our knowledge, this is the first case of GCT in the cecum treated by ESD in the West; all the other four cases were reported in China [5, 6].

