










Serviços Personalizados
Journal

Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
 Citado por SciELO
Citado por SciELO Links relacionados
 Similares em
SciELO
Similares em
SciELO Compartilhar

 Permalink
PermalinkActa Portuguesa de Nutrição
versão On-line ISSN 2183-5985
Acta Port Nutr no.9 Porto jun. 2017
https://doi.org/10.21011/apn.2017.0903
ARTIGO DE REVISÃO
Bioethical principles and nutrition in palliative care
Princípios Bioéticos e Nutrição em Cuidados Paliativos
Joana S de Andrade1*; Mariana Magalhães Almeida1; Cíntia Pinho-Reis2,3
1Faculdade de Ciências da Saúde da Universidade Fernando Pessoa, Rua Carlos da Maia, n.º 296, 4200-150 Porto, Portugal
2Unidade de Cuidados Continuados da Fundação Fernando Pessoa, Hospital-Escola da Universidade Fernando Pessoa, Avenida Fernando Pessoa, n.º 150, 4420-096 Gondomar, Portugal
3Instituto de Bioética da Universidade Católica Portuguesa, Rua Diogo Botelho, n.º 1327, 4169-005 Porto, Portugal
Endereço para correspondência
ABSTRACT
The last few decades have been witness to huge advances in medical technology and, consequently, in Ethics. One area that reflects this progress has been the area of food, nutrition and hydration in Palliative Care. The current review focuses on the overall knowledge about Ethics in the field of Nutrition in Palliative Care regarding the principles of autonomy, beneficence, non-maleficence and justice.
Keywords
Bioethical principles, End of life, Ethics, Nutrition, Palliative care
RESUMO
As últimas décadas têm sido palco de inúmeros avanços na tecnologia médica e, consequentemente, na Ética. Uma das áreas que reflete estes progressos é a área da alimentação, nutrição e hidratação em cuidados paliativos. A presente revisão foca-se no conhecimento global relativamente à Ética na Nutrição em Cuidados Paliativos relativamente aos princípios de autonomia, beneficência, não maleficência e justiça.
Palavras-chave
Princípios bioéticos, Fim de vida, Ética, Nutrição, Cuidados paliativos
INTRODUCTION
Since the discovery of DNA by Watson and Crick (1952), there has been a medical and a technological revolution that brought the need to explore a new ethical world, so that Bioethics has emerged as a new domain of reflection and practice in the healthcare area (1-3), including nutrition.
Ethics is the science of morality. In its etymological sense, it is a word that comes from the Greek ethos, which has two forms: the first word, êthos, refers to the way of being, to the character, to the inner reality from which human acts originate. The second word, ethos, indicates customs, habits or habitual action (4).
Medical advances, increasing longevity and prevalence of chronic and progressive diseases have contributed to a significant increase of patients outside the therapeutic possibilities of healing, which has led to the need for the existence of Palliative Care (PC) (5, 6).
PC is an active, total care of the patients whose disease is not responsive to curative treatment. PC is interdisciplinary in its approach and encompasses the patient, the family and the community in its scope. It sets out to preserve the best possible quality of life (QoL) and comfort until death. PC is a human right. It promotes a holistic approach to patients and family members because it palliates not only physical or psychological symptoms but also social and spiritual problems. The main goal of PC is to provide comfort and QoL to patients suffering from severe incurable disease at an advanced and progressive stage, as well as to their families. This may be achieved through prevention and alleviation of physical, psychological, social and spiritual suffering, helping the patient to live through their illness the best way possible, while ensuring that the patient maintains a life that is as active as possible until death (7-16).
The World Health Organization (WHO) also defines PC with the statements that death is a natural process and PC neither abbreviates nor prolongs life through euthanasia or therapeutic obstinacy, as it seeks to alleviate pain and other symptoms (2). PC provides individualized and humanized inter- and multidisciplinary care, with respect for the scientific knowledge but also the patient’s values, beliefs and practices, to preserve and guarantee the best comfort, wellbeing, dignity and QoL possible until death (3, 6-11, 13-16).
Food, nutrition and hydration play a key role in PC (3, 14). Scientific literature states that food has not only a physiological meaning but also a symbolic value, affecting our psychological and emotional status, based on our cultural and spiritual beliefs. When nutritional support in PC is established, the patient’s best interest must be safeguarded. For some authors, nutrition support (NS) is a basic human care and as long as the patient wants to and can be fed, there is an obligation to provide such measure. Other authors consider NS constitutes a medical treatment and that there are circumstances in which it is legitimate for them not to start, maintain or stop it (3, 14, 17, 18). So food, nutrition and hydration represent the most controversial issue in the area of care, because it creates conflict among the principles of autonomy, beneficence, non-maleficence and justice (14).
- Bioethical principles
The U.S. National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research has established, in the Belmont Report, three bioethical principles – autonomy, beneficence and justice (19). Later, Beauchamp and Childress developed the concepts of autonomy, beneficence, non-maleficence and justice. These principles, combined with technical and scientific knowledge, must be applied in nutrition practice, and these should be the guiding principles to health care actions, since they contain most of the moral issues that arise in health care (7, 20).
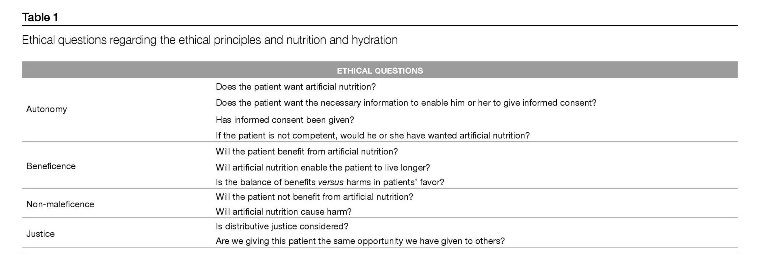
According to Beauchamp and Childress, Ethics describes how society understands and examines moral life in terms of decision-making. The four principles stated above find their roots in the history of philosophy and in the tradition of medical ethics, from which they gain their justification as principles. They do not obey any hierarchical order and they are valid prima facie. In the event of conflict between them, the situation in question and its circumstances shall define what will give precedence (1). There are also several ethical questions about the ethical principles that healthcare professionals must address regarding decision-making (Table 1 ).
1.1. Autonomy
There is a common understanding of the meaning of this word:
self-determination to choose or refuse any treatment at any stage of the disease, even if it leads to one’s death (2, 7, 10, 14, 16, 17, 19-23). So, the principle of autonomy recognizes a patient’s right and ability to make a personal choice (2, 10, 19-21). Informed consent is necessary to promote autonomy, protect patients from unwanted artificial nutrition and hydration (ANH) and enable decisions to be made that are consistent with patients’ values and culture. The ability to give informed consent is central to the decision-making process. So, if patients reject a treatment, patients’ wishes take precedence over the healthcare team’s duty of beneficence (10, 24). However, this depends on patients’ ability to give consent because sometimes patients have no decision-making capacity, due to illness, treatments, mental problems, or some kind of restriction to their freedom (2, 10, 19-21).
Despite the fact that a patient in unable to make his own decision, if he, by means of a living will or proxies, expresses his wishes regarding treatments, even in the face of family refusal, healthcare professionals must respect his earlier decision, since it was taken in a time when decision-making was possible (3, 10, 21, 25). However, if the individual does not have any of the above and no decision-making ability, healthcare professionals must take the decision considering patients’ best interest, avoiding paternalism but preserving (10, 21, 22) their patients’ integrity and dignity while respecting their vulnerability (26, 27, 28). It is important to understand that an autonomous decision needs the full understanding of the procedures and its consequences and also must be voluntary, without the presence of coercive or persuasive measures (29).
While the principle of autonomy is highly valued in Western culture, it should be balanced with the principles of beneficence, non-maleficence and justice (7, 22).
1.2. Beneficence
The term beneficence comes from the Latin bonum facere, which means, “do good”. The Hippocratic Code established that healthcare professionals have the obligation to do good to the ill person according to their skills, understanding, knowledge, reason and ability to judge and decide (30).
Beneficence implies that the treatment will be in the patients’ best interests and will benefit them (2, 14, 19-21). Patients should not be exposed to risk or extra suffering unless there is a reasonable expectation of a proportional benefit (10, 31). Regarding artificial nutrition and hydration, if the risks and burdens of a treatment outweigh the benefits, it is imperative to withdraw or withhold the nutritional support (10). It is also vital to prevent or remove harm and promote the patient’s wellbeing (19).
Putting into practice the principle of beneficence is quite challenging, because this principle is constantly in conflict with the principle of the respect for autonomy that guides healthcare professionals to always act with the informed consent of a free moral agent (2, 14, 17, 18, 24).
1.3. Non-maleficence
The Hippocratic Code refers to this principle as primum non nocere “above all do not harm” (10, 19, 20, 21, 23). Thus, non-maleficence acts to minimize potential or actual harm (2, 17, 19, 20). According to Beauchamp and Childress, it means that health professionals should not kill, disable, cause pain, offend or deprive others of the goodness of life (19).
The concept of this principle can raise issues when treating a patient may be disproportionate, and maintaining treatment may cause further suffering – maleficence. As this paradox is commonly encountered in practice, the concept of dual effect becomes important. This suggests that performing an act that brings about a good consequence may be morally right even though this may be achieved only at the risk of harmful side effects. Regarding NS, the principle of dual effect is apparent when meeting nutrition or hydration needs also results in harmful effects such as fluid overload or aspiration pneumonia. In this case, there is a need to establish the difference between food and fluids from nutrition and hydration by artificial means, since these actions are morally different (24).
Beauchamp and Childress also distinguish between withheld and withdrawn life-sustaining interventions such as artificial nutrition and hydration, since both situations are associated with different senses of responsibility. If withdrawn is the option, the person who makes the decision feels responsible for the consequences of that action. However, in a situation of not beginning artificial nutrition and hydration, the healthcare professional no longer feels this responsibility (32). This happens because the withdrawal of treatment is not closely associated with death from thirst and starvation; instead, it is associated with the natural course of the disease (14).
1.4. Justice
This principle suggests that every patient has equal right to receive nutrition and hydration and that decisions about how resources are applied must be made in the fairest possible way – equity regardless of his ethnicity, social or economic status (10). It also infers that adequate time should be taken to ensure that appropriate decisions are made. So, Nutritionists are, therefore, faced with the difficulty of balancing the principle of justice against beneficence and autonomy, while attempting to deploy limited resources to maximum benefit (2, 10, 14, 17, 19-21, 23, 31).
- Artificial Nutrition and Hidratation in Palliative Care – Treatment or Basic Human Care
Ethical issues surrounding food and fluids are complex because there is not only a physiological side but also a psychological side that is affected (13, 14, 17, 22, 33, 34).
In general, when nutritional support in PC is established, the patient’s best interest should be safeguarded. Thus, decisions must be made taking into account all the necessary ethical aspects, especially with regard to the ethical principles of autonomy, beneficence, non-maleficence and justice (3, 13).
One of the most controversial areas in PC is Artificial Nutrition and Hydration. In some cases, at the request of a capable patient, voluntary cessation of feeding may occur. In this context, all patients have the right to refuse food if this does not precipitate death more rapidly than the disease itself. In other cases, it is the multidisciplinary team itself that discusses whether ANH should be started, maintained or suspended (3).
One of the biggest controversies is whether ANH shall be considered medical treatment or basic care. For some authors, ANH is a basic human care and, as such, as long as the patient wants to and can receive Artificial Nutrition and Hydration, there is an obligation to provide him with the necessary means to do so (3, 8).
Some authors argue that, from the moment nutrition is administered by artificial means, it should be considered a treatment like any other and it should be subjected to weighting its proportionality and, as such, there are circumstances in which it is legitimate for them not to start, maintain or stop it (3, 8). With regard to this issue, some authors refer that, in some cases, initiating ANH will only prolong suffering and therefore it is legitimate to withhold or withdraw these measures (3). In some cases, the purpose of ANH is to postpone the loss of autonomy and guarantee dignified survival. At the same time, it prevents unnecessary malnutrition, ensuring that the patient receives enough nutrition to restore or maintain nutritional status while promoting wound healing and tissue repair (these patients are vulnerable to infection, respiratory problems and develop pressure ulcers) (3, 7, 11, 13, 14, 35).
Food and eating have not only a physiological side but also a strong symbolic value, because it affects our psychological and emotional status, based on our cultural, religious and spiritual beliefs (17, 34). Every religion has its own view when it comes to medical procedures and it is mandatory for the health professional to respect and act according to these beliefs (21).
- Religious and cultural views about Artificial Nutrition and Hydration
The Catholic Church differentiates the ordinary treatment from the extraordinary treatment, where the former is mandatory and the latter is disproportionate. When the treatment is not working or is damaging, it can be discontinued. However, there are different theories regarding this subject, even in the Catholic Church. Some Catholics think, as some ethicists do, that withholding ANH in PC is unethical because every human has a basic need for food and water. They feel that ANH is not a medical treatment but a basic care, as food and water are basic needs. So, withdrawing or withholding ANH is the same as killing the patient. Pope John Paul II (2004) held this view: he stated that providing food and fluids, regardless of how they are administered, is a natural way of preserving life and, as such, is a moral obligation and that withdrawing feeding tubes is “euthanasia by omission”. On the other hand, they are in favor of providing ANH as long as the benefits outweigh the risks (8-10, 15, 36, 37).
The Protestant Church has many doctrines in its different subgroups – some are very liberal and think that intolerable suffering and poor QoL may justify measures to hasten death, withholding or withdrawing Artificial Nutrition and Hydration; others believe that nutrition and hydration are a basic care and should not be stopped (10).
The Jewish religion distinguishes between active and passive actions and, therefore, between withholding and withdrawing Artificial Nutrition and Hydration, so it permits the withholding (if this is the patient’s wish) but forbids the withdrawing. For conservative and orthodox Jews, treatments that have been started cannot be stopped, and food and drink are considered basic needs and not treatments. Orthodox Jews also believe that a patient can ask for ANH and it should be given to him if the advantages outweigh the harms (9, 10, 15).
While Islam contemplates food and hydration as basic care and not medical treatment, it can be withdrawn or withheld if there is an informed consent (10).
As in different religions, different cultures also have diverse points of view on this subject: for example, suffering in some cultures is considered an important aspect of the human experience, and certain interventions might not be restrained, even if they are painful. For some people, every moment of life, no matter how painful and limited, is of inestimable value (22, 33). Seeing the patient as an individual, actively listening to the patient, reaching an agreement with an understandable explanation of symptoms or illnesses and presenting treatment are all specific ingredients essential to successful decision-making about ANH (with the patient himself or his family) (13, 38, 40).
- Risks and benefits of Artificial Nutrition and Hydration
ANH is subject to considerable risks that may negatively contribute to the patient’s comfort, QoL, well-being and survival. If the option is enteral nutrition, nasogastric tubes may cause aspiration pneumonia, particularly in debilitated patients, diarrhea, vomiting and esophageal perforation; percutaneous endoscopic gastrostomy can cause nausea, vomiting, and others (3, 7, 8, 13, 14, 22, 39).
If Parenteral Nutrition becomes an option, the use of central venous catheters may cause pneumothorax, bleeding and infection, and even the use of peripheral venous catheters may result in pain and infection (3, 4, 7, 11, 13, 31, 35). Additionally, in patients with profound change or absence of renal function, fluid administration may cause peripheral or pulmonary edema (7, 17, 40).
CRITICAL ANALYSIS AND CONCLUSIONS
Regarding the considerations about Bioethical Principles, it is extremely important to develop and encourage discussion surrounding end-of-life nutrition and hydration. The four bioethical principles raise very important issues in the area of nutritional support in PC, especially from the Nutritionists’ perspective. The principle of autonomy should be strongly respected, because the patient has the right to decide what nutritional care he wishes to receive or not. In this context, considering patients are competent and that their consent is based on adequate information, their decision should be respected. The principle of beneficence on which healthcare professionals must act, accordingly to the patients’ benefit, applies the same kind of thinking. It is necessary to address all these issues early and proactively, informing the patient and family members that, in some situations, prolonging life may increase discomfort and is considered therapeutically futile. With regard to the principle of non-maleficence, if ANH does not cause benefit, it should be suspended or not started, even though this situation is still regarded as abandoning the patient, leaving him to die of hunger and/or thirst. Concerning the principle of justice, every patient has the right to be offered the same treatment opportunities.
Decision-making regarding ANH in PC interfere with feelings, emotions and attitudes. On various occasions, healthcare professionals are faced with their own professional dilemmas and with the fear of being accused of killing or letting someone die. Legally, withdrawing and withholding treatment are indistinguishable; yet many patients, families, and physicians find removal to be more emotionally charged. Health professionals need to accept and understand the philosophy and principles of PC and overcome their fears in relation to this area of care. It should be emphasized that, even if ANH is suspended or not started, this does not mean neglect or abandonment of the sick person, as holistic PC will continue to be provided, promoting comfort and QoL until death. There is a strong need to develop and encourage the debate on these issues in order to make them more consensual and improve decision-making and the assistance of healthcare professionals to patients in PC.
After completing this review, we observed that the same ethical issues referred to decades ago are the same today; there was no development in the area of end-of-life nutrition and hydration. However, in many cases, food will not always promote comfort and wellbeing. The undesirable effects of nutrition techniques, especially artificial nutrition, are sometimes causes of worsening QoL, damaging the real objective of PC. The current practice of the Nutritionist should be to weigh all their intervention from the point of view of risks and benefits, and the benefits of NS should always outweigh the risks. All risks and benefits should be discussed in advance with the patient and his family, taking into account their desires and needs. There is a lot of work to be done and it is imperative that Nutritionists possess in-depth knowledge about clinical nutrition, medicine, cultural and religious values, health care and law, good communication skills and empathy with patients and family members. Above all, Nutritionists as a professional class must define their clinical and ethical skills in the ethical field of NS in palliative and end-of-life care.
REFERENCES
Joana S de Andrade
Rua 20, n.º 995,
4500-264 Espinho, Portugal
Recebido a 22 de fevereiro de 2017
Aceite a 7 de junho de 2017


{kind=link}