










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkGE-Portuguese Journal of Gastroenterology
versão impressa ISSN 2341-4545
GE Port J Gastroenterol vol.25 no.4 Lisboa ago. 2018
https://doi.org/10.1159/000481176
IMAGES IN GASTROENTEROLOGY AND HEPATOLOGY
Fleeting Angiodysplasia
Angiodisplasia fugaz
José Pedro Rodrigues, Joyce Chivia, Pedro Cardoso Figueiredo
Gastroenterology Department, Hospital de Egas Moniz, Centro Hospitalar Lisboa Ocidental, Lisbon, Portugal
* Corresponding author.
Keywords: Quality in endoscopy, Angiodysplasia, Vasoconstriction
Palavras-Chave: Qualidade em endoscopia, Angiodisplasia,·Vasoconstrição
Vascular malformation of the gastrointestinal tract is an uncommon, but not rare, cause of gastrointestinal bleeding [1]. Indeed, especially in the elderly, angiodysplasia represents the most frequent cause of small bowel bleeding [2]. In the colon, the prevalence estimates vary widely, from <1% in asymptomatic patients to 2–40% in the setting of low gastrointestinal bleeding [3]. The burden is particularly high when considering patients evaluated for obscure gastrointestinal bleeding who ultimately are found to have non-small-bowel lesions within reach of conventional endoscopy. Published series report amissing lesion rate reaching up to 25% and the majority were vascular lesions [4].
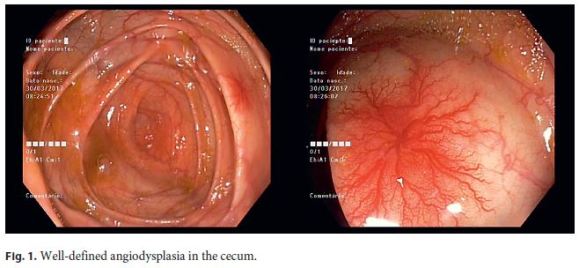
We present the case of a 55-year-old male patient, with no relevant previous medical history, who underwent a total colonoscopy for iron deficiency anemia evaluation, which in the cecum identified a 15-mm well-defined angiodysplasia (Fig. 1). To improve colon cleansing, water was flushed over the vascular lesion. The consequence was attenuation of the lesion, making it almost imperceptible at a distance (Fig. 2). Argon plasma coagulation was still used for ablation of the angiodysplasia, and the hemoglobin level has remained stable since then (Hb 13 g/ dL, 3 months of follow-up after iron replacement).
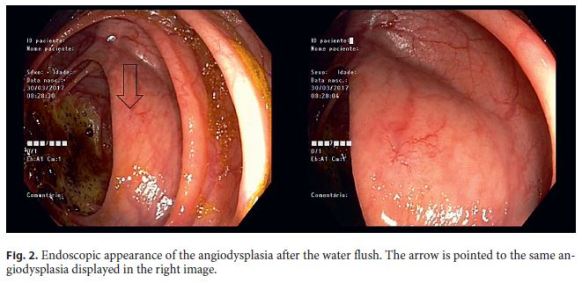
The reported case demonstrates one possible reason for missing vascular lesions in the colon as the vasoconstriction caused by the water flush, turned the lesion almost indistinguishable from the surrounding colonic mucosa.
References
1 Szilagyi A, Ghali MP: Pharmacological therapy of vascular malformations of the gastrointestinal tract. Can J Gastroenterol 2006;20:171–178. [ Links ]
2 Gerson LB, Fidler JL, Cave DR, Leighton JA: ACG clinical guideline: diagnosis and management of small bowel bleeding. Am J Gastroenterol 2015;110:1265–1287. [ Links ]
3 Strate LL: Lower GI bleeding: epidemiology and diagnosis. Gastroenterol Clin North Am 2005;34:643–664. [ Links ]
4 Tee HP, Kaffes AJ: Non-small-bowel lesions encountered during double-balloon enteroscopy performed for obscure gastrointestinal bleeding. World J Gastroenterol 2010;16:1885–1889. [ Links ]
Statement of Ethics
This study did not require informed consent nor review/approval by the appropriate ethics committee.
Disclosure Statement
The authors report no potential conflict of interest.
* Corresponding author.
Dr. José Pedro Rodrigues
Gastroenterology Department, Hospital de Egas Moniz
Centro Hospitalar Lisboa Ocidental
Rua da Junqueira 126, PT–1349-019 (Lisbon)
E-Mail jp.azevedo.rodrigues@gmail.com
Received: July 10, 2017; Accepted after revision: August 30, 2017
Author Contribution
All authors have read and approved the manuscript being submitted. All authors listed contributed significantly to the work.

