











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
86-year-old male, non-smoker, medical history of cardiac failure and chronic kidney disease, presented at emergency department with 8-month evolution of dyspnea and dry cough, progressively worsening. On examination the patient had tachypnea, oxygen saturation of 85% on air and diffuse crackles in lower lung area. Chest radiography showed bilateral inferior opacities. He was admitted for pneumonia with hypoxemic respiratory failure and completed antibiotic treatment, without recovery. Chest computed tomography (CT) scan showed fibrosing interstitial lung disease (ILD), suggestive of non-specific interstitial pneumonia pattern. The patient developed rapid clinical deterioration with circulatory shock. In spite of responding to vasoactive agents, he maintained dyspnea and extensive cervical and thoracic subcutaneous emphysema was noticed. He repeated a chest-CT scan revealing subcutaneous emphysema, bilateral pneumothorax (Fig.1 A-B, blue and yellow arrows, respectively) and an exuberant pneumomediastinum, with new inferior ground glass opacities (Fig.1C-D, red arrow and asterisk), meaning ILD exacerbation. He had no indication for invasive measures and progressed with rapid deterioration and death.
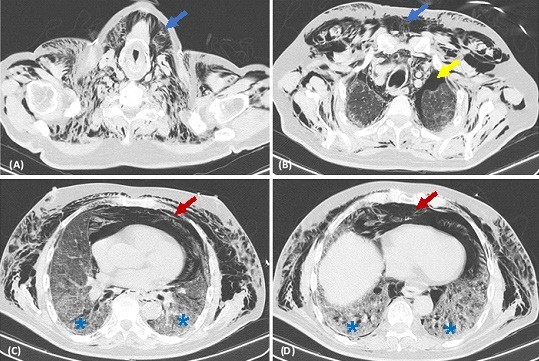
Figure 1: (A) and (B) Axial chest-CT scan image showed cervical and thoracic subcutaneous emphysema (blue arrows), and apical bilateral pneumothorax (yellow arrow). (C) and (D) Axial chest-CT scan image showed an exuberant pneumomediastinum (red arrows) and new inferior ground glass opacities (asterisks), superimposed to fibrosing nonspecific interstitial pneumonia pattern, meaning ILD exacerbation.
Pneumomediastinum is usually a benign condition, with treatment directed to symptoms relief. Increase in alveolar pressure lead to rupture of the alveoli, causing dissection of air along peribronchial and perivascular sheets.1 In cases of underlying pulmonary fibrosis, rupture of blebs and cysts contribute to the development of this condition.1,2
Given the changes in pressure gradients, the air can dissect to subcutaneous tissue and also pass to the pleura resulting in subcutaneous emphysema and pneumothorax, respectively.2 In rare cases, pneumomediastinum may adversely progress to continuous accumulation of air, with vascular and tracheal obstruction, leading to fatal cardiac tamponade.1,2

