











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Stroke is classically characterized as a neurological deficit resulting from an acute focal lesion of the central nervous system from vascular causes, including cerebral infarction, intracerebral hemorrhage, and subarachnoid hemorrhage 1,2. Impairments in cognitive function usually accompany the occurrence of stroke in people’s lives with an impact on daily life 3,4, which are manifested in the 3-6 months after stroke 5. Post-stroke cognitive impairments are currently the most disabling after-effects 6, with a prevalence of 16-53%, with approximately 10-20% of strokes being hemorrhagic and the remainder ischemic 7. A 2011 study reported that worldwide, stroke is responsible for about 5.5 million deaths annually 8. Evidence shows that one of the ways to reduce cognitive impairment is through cognitive rehabilitation, as it impacts even patients with chronic conditions. Cognitive rehabilitation can be accomplished in several ways, including through physical activity 9, since the regeneration of motor and cognitive functions is based on the plastic properties of the central nervous system and compensatory strategies to recover lost functions 10. Evidence shows that physical activity improves muscle function, motor skills, cardiorespiratory function, and metabolic regulation 11-14.
Further, it decreases anxiety and depression levels and increases self-esteem 15, promotes social integration and the learning of social rules 16, and improves global cognitive functions 17. It is well known that blood flow and oxygenation in cortical regions are influenced by the intensity of the exercise session 18,19. Further, increased prefrontal cortex oxygenation may indicate greater cortical activity, leading to enhanced cognitive processes such as working memory and attention 18,20. There is a consensus that physical activity is associated with a lower risk of stroke and mortality, as it is a potential preventive measure against cognitive decline 21.
Although a growing body of literature addresses the effect of physical activity on cognition, few address the post-stroke physical activity prescription and the impact of physical activity on post-stroke cognitive performance 21. In a review, Barker and Eickmeyer 22 present general guidelines for physical activity, where the recommendation is that adults perform aerobic physical activity, emphasizing resistance or strength training, twice a week. Another study by Gambassi et al. 23 addresses resistance training for motor recovery of patients with stroke. Further, in a recent study, Izquierdo et al. 24 explain that the ideal prescription of exercises for preventing or treating dementia has yet to be defined.
There needs to be more literature clearly describing which type of physical activity training program is adequate to reduce post-stroke cognitive impairment and optimize recovery. Should the training program be isolated or combined? What should its duration, intensity, and weekly frequency be? In this context, an isolated intervention program is considered when only one type of activity is used during all interventions; in this case, only aerobic activity can be used, or resistance activity, strength activity, or postural balance, among others. When it comes to combined physical activity, there is a combination of physical activity, which can be aerobic with resistance or strength activity, among others. For example, in this line, it is known that aerobic activity improves cardiorespiratory fitness, increases the expression of neurotrophic factors, and increases hippocampal size 4,25; resistance activity increases muscle mass, strength, and power and improves executive function and selective attention 4,26; and strength activity enhances bone mineral density and neuromuscular performance, increases proteins involved in neuronal survival and synaptic plasticity in the hippocampus, improves memory 27,28. Thus, considering the gains each type of activity could bring the participants, a program that combines different types of activity per session throughout an intervention program might be even more efficient. Concerning duration, we find a variation of 1 day to more than a year. As for exercise intensity, there is also a variation from low to moderate to high intensity 29-31. This shows that there is still debate about the type of physical activity program, ideal duration, and exercise intensity to lead to therapeutic benefits after stroke. Thus, this review aimed to evaluate the effects of physical activity programs on the cognition of patients with stroke, comparing the effectiveness of isolated or combined rehabilitation training programs and the duration and intensity of training to identify the most effective training programs for post-stroke cognitive rehabilitation.
Methods
Population
Men and women 18 years of age and older with acute or chronic stroke in various stages participated.
Intervention
All types of physical activity for patients with stroke rehabilitation, defined as any bodily movement produced by the skeletal muscles that results in energy expenditure above resting levels, are performed in isolation or combination with other activities. There is no restriction on the duration of intervention programs, intensity, and frequency.
Comparator
Any type of activity was used as a control, from usual care, recreational activities, cognitive training, or even physical activity.
Outcome
Studies that assessed cognition in its various domains (such as attention and concentration, executive functions, memory, language, visuospatial ability, abstract thinking, calculation, and orientation) using either neuropsychological testing or imaging were included.
Study Design
Only randomized controlled trials were included. Non-experimental studies, single experimental designs, review and opinion articles, studies not published in English, and those published before 2013 were excluded.
Search Strategy
On April 12, 2023, the first author searched five databases, namely PubMed, Web of Science, Scopus, and SPORTDiscus, using the following search words and Boolean operators: (“physical training” OR exercise OR “physical activity” OR “physical intervention”) OR (“physical training” OR exercise OR “physical activity” OR “physical intervention”) AND (“Cognitive Rehabilitation” OR Cognition) OR (“Cognitive Rehabilitation” OR Cognition) AND (CVA OR Stroke OR “cerebrovascular accident”) OR (CVA OR Stroke OR “cerebrovascular accident”). In the PEDro database only, we used the following search terms: cognitive*, aerobic*, and stroke*. We also searched the reference lists of all included studies to identify any other studies that our search strategy might have missed. We used a combination of medical subject title (MeSH) terms where available, free text search terms, and Boolean operators. MeSH search terms using “Exercise,” “Cognition,” and “Stroke” were combined with “physical training” OR exercise OR “physical activity” OR “physical intervention,” “Cognitive Rehabilitation” OR “Cognition,” and “CVA OR Stroke OR “cerebrovascular accident.” Additionally, a manual search of peer-reviewed articles on the cognitive benefits of physical activity after stroke, considering the type of intervention program (combined or isolated, i.e., a combination of different types of physical training or a single type of physical training activity) and duration, was also performed to locate potentially eligible studies for inclusion in the review 32.
Selection Process
All studies were imported into Excel using Zotero (reference management software), facilitating screening and eliminating duplicate records. The three investigators conducted a comprehensive search of studies, independently reviewed titles and abstracts of the imported registries, and discussed inconsistencies until a consensus was reached. Then, two researchers independently examined the titles and abstracts of all articles retrieved. In case of disagreement, consensus on which reports to display in full-text was reached through discussion. If necessary, the third researcher was consulted to make the final decision. Subsequently, two researchers independently screened the full-text articles for inclusion. Again, in case of disagreement, consensus on inclusion or exclusion was reached through discussion, and, if necessary, the third investigator was consulted 33,34.
Data Collection and Extraction
Two reviewers independently collected information from eligible studies using the data extraction form based on Lumley et al. 35. A third reviewer arbitrated the discussion to resolve discrepancies between the two review authors. For each study, information collected included descriptive details about the first author’s last name and year of publication, study design and period, study methods, study participants (age group, eligibility criteria), interventions (type, duration, intensity), and outcome data.
Study Risk of Bias Assessment
The risk of bias for each study was assessed using the Cochrane Risk of Bias (RoB 2.0) tool 33,36. Domains in this checklist include: (1) selection bias (including random sequence generation and allocation concealment); (2) performance bias (including participant concealment); (3) detection bias (including blind assessment); (4) attrition bias (including incomplete result data); (5) reporting bias (including reporting of selective results); and (6) other biases (any other bias observed). Two reviewers independently applied the tool to each included study and recorded supporting information and justifications for judgments of risk of bias for each domain (low, some concerns, and high). The lack of consensus on the risk of biased judgments was resolved by discussion to reach an agreement between the two review authors, with a third review author acting as arbiter when necessary.
Results
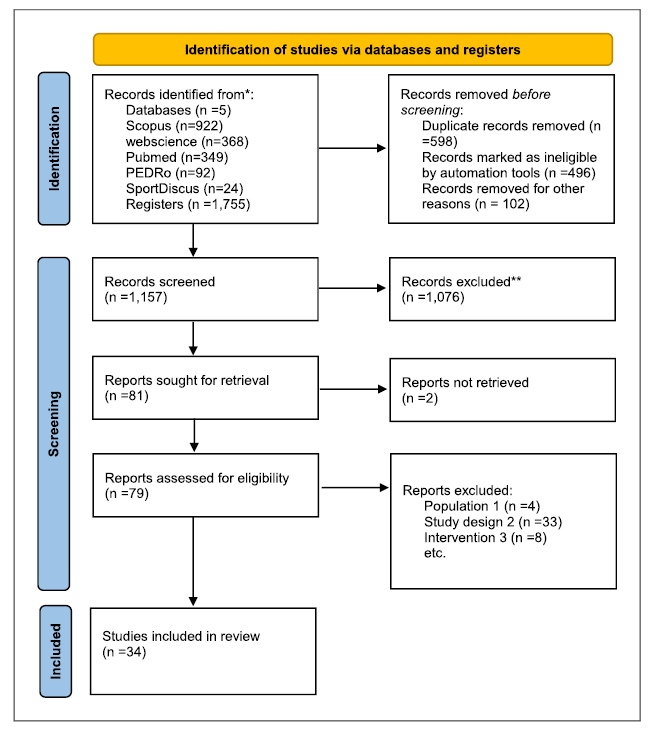
In the five databases searched, we found 1,755 records: 922 in Scopus, 368 in Web of Science, 349 in Pubmed, 92 in PEDRo, and 24 in SPORTDiscus. After removing duplicates, we examined 1,157 records, reviewing 79 full-text documents. Subsequently, we searched for documents that cited any of the initially included studies and the references of the included studies. However, no extra articles meeting the inclusion criteria were found in these searches, as shown in the flow diagram in Figure 1.
Study Characteristics
The studies included in the review present data collected in thirteen countries on three continents (online suppl. Material 1; for all online suppl. material, see https://doi.org/10.1159/000535272). We found fourteen studies in Asia, twelve studies in Europe, and eight studies in America.
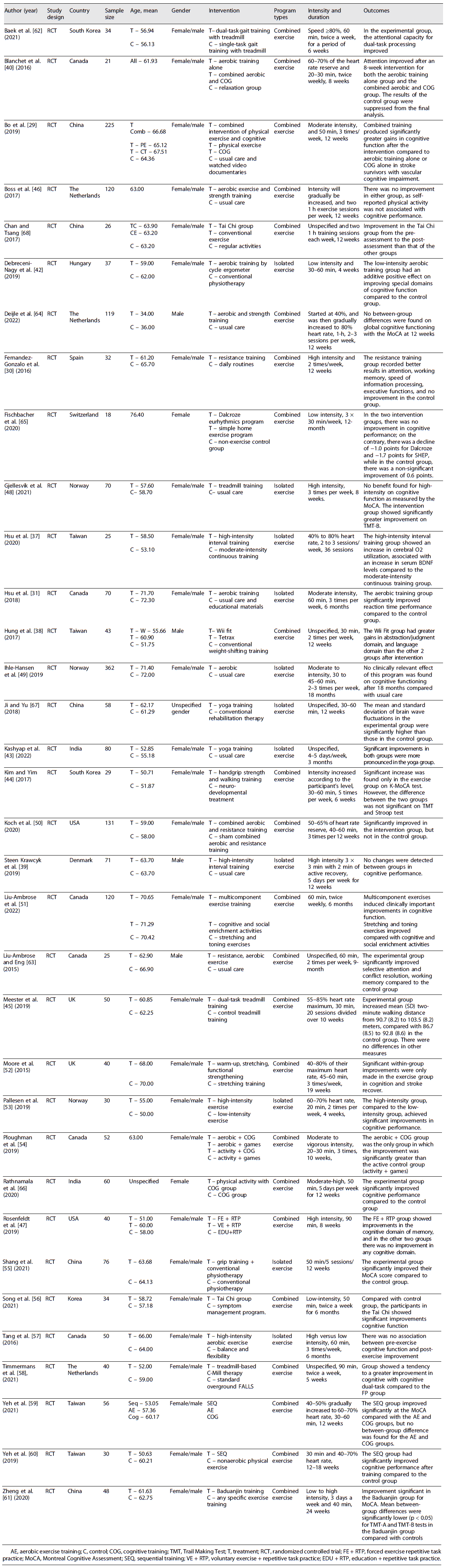
We included a total of 34 randomized controlled trials, of which three were double-blind 37-39, 22 were single-blind, and the remaining nine, although obeying randomization of participant recruitment, did not present any information about the concealment process, both for the participants and the evaluators. The sample size in the studies ranged from 18 to 362 participants. The mean age of the participants in the reviewed studies was 61.91 years. Concerning sex, 27 included men and women in their sample 29-31,37,40-62, four had a sample composed only of men 38,39,63,64, two composed only of women 65,66, and one did not specify the gender in its sample 67. Regarding the types of exercises targeted at the intervention groups, the combined rehabilitation training programs involved: dual-task gait training 45,58,62, aerobic and cognitive training 29,40,54,59,60,66, aerobic activity and strength activity 44,46, Tai Chi 41,56, aerobic and endurance training 30,50,63,64. The isolated aerobic training programs involved: aerobic training 31,42,48,49, high-intensity training 37,39,53,57, and yoga training 43,67. On the other hand, the control groups participated in programs involving single-task gait training with a treadmill 45,62, performing conventional exercises 29,31,38,39,42,43,46,48,49,55,63,64,67, daily routines 30,41,61,65, which included mobilization of upper and lower limbs, stretching and muscle strengthening with elastic bands and walking 51,52. An overview of the study and participant characteristics is listed in Table 1.
Risk of Bias in Studies
We note that of the 34 studies reviewed, sixteen had a low risk of bias, eleven had a high risk, and seven presented some concerns, as illustrated in Figure 2.

Results of Syntheses
Of the 34 included studies, 23 used three types of combined rehabilitation training programs, essentially involving combinations of aerobic and cognitive training, aerobic exercise and strength training, and aerobic and resistance training. The remaining 11 studies used isolated rehabilitation training programs primarily involving aerobic exercise (online suppl. Material 2).
Cognitive Function Outcome Measures
Regarding the use of neuropsychological instruments at baseline, of the 23 studies that used a combined rehabilitation training program, only 13 assessed cognitive function as shown in online supplementary material 3, with cases using a single test 29,41,50,61,63,65, two tests 38,44,46,51,59,64, and three tests 52. In the 11 studies using an isolated rehabilitation training program, 10 assessed cognitive function, either using a single test 37,48,53,57,67, two tests 39,49,55, three tests 31, or four tests 42.
Global Cognitive Function
Of the 23 studies that used combined rehabilitation training programs, only seven reported global cognitive functions assessed by neuropsychological tests 46,50,51,60,61,63,64, as detailed in online supplementary material 3. Of these, three reported significant improvements in the intervention group but not in the control group 50,51,60, and only three reported no between-group differences in global cognitive functioning 46,61,64. One reported significant improvements in the control group but not in the intervention group 63. Of the 11 studies that used an isolated rehabilitation training program, only three documented global functions 31,48,49. One study reported significant improvements in the intervention group but not the control group 31. In contrast, the other two reported no relevant benefit of this program in cognitive functioning 48,49, as shown in Table 1.
Specific Domains of Cognition
Memory
Ten studies using a combined rehabilitation training program reported memory outcomes assessed by neuropsychological tests 29,30,40,46,47,50,52,58,63,66, as shown in online supplementary material 3. Of these, eight reported significant improvements in the intervention group but not in the control group 29,30,47,50,52,58,63,66, and only one 46 reported that self-reported physical activity was not associated with cognitive performance. However, one study reported no significant effects for short delays in working memory (Brown-Peterson paradigm: p = 0.92) or episodic memory (revised Hopkins Verbal Learning Test: p = 0.26) 40. Of the 11 studies that used a rehabilitation training program alone, six reported on memory 39,42,48,53,55,57. Of these, only one reported improvements in the intervention group but not in the control group 55, two reported no significant effects of the intervention in both groups 42,53, and three 39,48,57 showed no evidence of the impact of a rehabilitation training program alone on memory in patients with stroke, as shown in Table 1.
Attention
Ten studies that used a combined rehabilitation training program assessed attention using neuropsychological testing 30,40,44,46,51,56,59,61,63,66, as illustrated in online supplementary material 3. Of these, eight reported improvements in the intervention group. Still, not in the control group 30,40,44,51,56,59,63,66, one reported no significant difference between the Baduanjin group and the controls for attention 61, and a single one (46) did not report improvements. The seven studies that used a stand-alone rehabilitation training program also assessed attention using neuropsychological tests 31,39,43,48,53,55,57. Of these, four showed improvement in the intervention group but not in the control group 31,43,53,55, and three did not report any improvement 39,48,57, as shown in Table 1.
Visuospatial Ability
Four studies using a combined rehabilitation training program assessed visuospatial ability 56,59-61, as depicted in online supplementary material 3. Three reported improvements in the intervention group but not in the control group in visuospatial ability 56,59,60, and one reported no significant difference between the Baduanjin group and the controls 61. Three other studies that used a stand-alone rehabilitation training program also assessed visuospatial ability 39,43,48. Of these, one reported improvements in the intervention group but not in the control group 43, and two reported no improvements at all 39,48, as shown in Table 1.
Language and Processing Speed
Of the five studies that used a combined rehabilitation training program, one assessed language 56, and the remaining studies assessed processing speed 30,50,61,66, as illustrated in online supplementary material 3. In five studies that assessed language and processing speed, four reported improvements in the intervention group but not in the control group 30,50,56,66, and one reported no significant differences between the Baduanjin group and the controls for processing speed 61. Of the five studies that used a stand-alone rehabilitation training program, two considered language 39,48, and both did not show improvement. For the remaining three studies, which also used a rehabilitation training program alone, they assessed processing speed 42,49,53, with improvements in the intervention group but not in the control group 42,53 and without improvements 49, as depicted in online supplementary material 3.
Executive Functions
Nine studies that used a combined rehabilitation training program assessed executive functions through neuropsychological tests 30,41,46,50,51,56,59,61,62, as shown in detail in online supplementary material Table 3. Eight of these nine studies reported improvements in the intervention group but not in the control group after the intervention; only one 46 did not report gains. Seven studies assessed executive functions 31,39,48,49,53,55,57 regarding the isolated rehabilitation training program. Of these studies, three showed improvements in the intervention group but not in the control group after the intervention 31,53,55, while four showed no improvements 39,48,49,57, as shown in Table 1.
Type of Intervention Programs
Regarding the type of rehabilitation training program, of the 23 studies that used combined rehabilitation training programs, 20 recorded cognitive improvements after completing the recommended exercise sessions 29,30,38,40,41,44,45,47,50-52,54,56,58-63,66, while three did not record cognitive improvements 46,64,65. Concerning the 11 studies that followed an isolated rehabilitation training recovery program, seven reported cognitive improvements 31,37,42,43,53,55,67, and four reported no cognitive improvements 39,48,49,57 (online suppl. material 4).
Regarding the type of exercise most used in each rehabilitation training program, we note that combined rehabilitation training programs used a combination based on strength physical activity in nine studies 38,41,44,47,51,52,56,61,64. In general, these studies included an active control group based on usual care 38,41,64, stretching and toning exercises 51,52, education, and repetitive task practice 47. One study included a passive control group, wherein the participants did not exercise or perform any other activity 61. Further, ten combined rehabilitation training program studies used aerobic physical activity 29,40,45,46,54,58,59,62,65,66 and included an active control group based on usual care 29,46, relaxation or activity with games 54,66, single-task gait training with treadmill 45,62, standard overground FALLS 58, aerobic exercise training and cognitive training 59,60; and resistance physical activity 30,50,63, wherein the control group used usual care 63, sham combined aerobic and resistance training 50, and daily routines 30. Concerning the isolated rehabilitation training programs, ten used aerobic physical activity 31,37,39,42,43,48,49,53,57,67, and the control group used usual care 31,39,42,43,48,49,57,67, moderate-intensity continuous training 37, low-intensity exercise 53, and only one study used strength exercise 55, and his control group received usual care. Most included studies compared an experimental exercise intervention to standard care or an alternative intervention, as illustrated in online supplementary material 5.
Duration of the Intervention Programs
The duration of the rehabilitative training programs varied from 4 weeks to a maximum duration of 18 months (49). Specifically for the combined training programs, we noticed a variation from less than 11 weeks 40,44,45,47,54,58,62 to more than 6 months 29,30,46,50-52,56,59-61,64,65. Studies lasting up to 11 weeks all reported improvements 40,44,45,47,54,58,62, the studies up to 6 months or more, nine registered improvements 29,30,50-52,56,59-61, and three did not register improvements 46,64,65. Concerning the isolated rehabilitation training programs, the duration ranged from less than 11 weeks 42,48,53,57 to more than 1 year 31,37,39,43,49,55,67, as depicted in online supplementary material 6. In studies lasting up to 11 weeks, two showed improvements 42,53, and two did not show improvements 48,57. Concerning studies lasting up to 1 year or more, five showed improvements 31,37,43,55,67, and two did not show improvements 39,49. As for the frequency with which rehabilitation training was carried out, we noted that there was a predominance of three times a week in 15 out of the 34 studies included, and the time spent for each session ranged from 20 min 40,53,54 to 90 min 47,58.
Exercise Intensity in Interventions
Regarding the intensity with which the exercises were performed, in the studies reviewed here, three presented low-intensity physical activity 42,56,65, twelve presented moderate-intensity physical activity 29,31,40,44,46,50,53,54,59-61,64, eleven presented high-intensity physical activity 30,37,39,45,47-49,52,57,62,66, and eight did not specify intensity 38,41,43,51,55,58,63,67. In studies with low-intensity physical activity, two recorded improvements 42,56, and one did not show improvements 65. In the studies using moderate-intensity physical activity, ten recorded improvements 29,31,40,44,50,53,54,59-61, and two did not register improvements 46,64. Concerning the high-intensity physical activity studies, seven reported cognitive improvements 30,37,45,47,52,62,66, and four did not record improvements 39,48,49,57. Regarding the studies that did not specify the intensity, all presented improvements 38,41,43,51,55,58,63,67.
Stroke Severity
Regarding stroke severity, in the studies reviewed here, 16 records involved participants with chronic stroke from 6 months to 1 year 30,31,43-46,48,51,52,54,55,57,58,60,63,65, 16 involved participants with subacute stroke 29,37-42,47,49,50,53,56,59,61,62,64, and two did not specify stroke severity of the involved participants 66,67. Regarding the studies in which the sample was composed of participants with chronic stroke, we noticed that 14 showed improvements 30,31,43-46,48,51,54,55,57,58,63,68, and only two showed no improvements 52,65. In studies in which the sample consisted of participants with subacute stroke, we noticed that 11 showed improvements 29,37,38,41,42,47,49,50,53,56,61 and five showed no improvement 39,40,59,62,64. Regarding the studies that did not specify stroke severity, all showed improvements 66,67.
Discussion
This review aimed to evaluate the effects of physical activity on the cognition of patients with stroke, comparing the effectiveness of isolated or combined rehabilitation training programs and the duration and intensity of training to identify the most effective training program for post-stroke cognitive rehabilitation. Thus, we systemized data that might allow for a recommendation for patients with stroke concerning the practice of physical activity safely and efficiently. Considering the potential benefits for cognition and mobility, since physical activity is linked to several physiological and neurological factors that promote longevity 69,70, participating in physical activity post-stroke rehabilitation should benefit protective and regenerative functions 71. However, considering the pre-defined eligibility criteria, there are still few published original studies with stroke rehabilitation programs using isolated and combined training, compared to a predominance of pharmacological therapies to lower blood pressure and conventional programs of muscle strength. Among the studies analyzed in this review, the combined rehabilitation training program appears to be more effective than the isolated rehabilitation training program, showing more significant improvements in several cognitive domains in the experimental group compared with the control group. One reason for this result is that the combined interventions offer favorable conditions for neuroplastic alterations due to the beginning of the synergy of action provided by the combination of physical activities 6 since each type of activity that intervenes in the combined training program has its specificity in terms of contribution. For example, it is known that aerobic exercise alone improves cardiorespiratory fitness and increases the expression of neurotrophic factors and hippocampal size 4,25. Resistance exercise, on the other hand, increases muscle mass, strength, and power and improves executive functions and selective attention 4,26,72. Moreover, strength exercise improves bone mineral density and neuromuscular performance, increases proteins involved in neuronal survival and synaptic plasticity in the hippocampus, and improves memory 27,28. The combined benefits of at least two types of physical activity thus have the potential to increase the cognitive benefits compared to an isolated physical activity.
There are also differences between the two rehabilitation training programs regarding the type of physical activity that each rehabilitation training program uses. In the combined rehabilitation training programs, we identified a predominance of combinations involving physical activity, as with physical activity of strength. Of these, eight studies that performed strength activity recorded cognitive improvements in the experimental group compared to the control group 38,41,44,47,51,52,56,61. Despite these widespread improvements in various cognitive domains, we also note a study 61 that found no significant differences between the Baduanjin group and controls about processing speed. This study tries to create a cause-effect relationship between attention and processing speed by explaining that for attention, there was a significant effect on the response time of a Go/No Go test 61, as processing speed is usually described in relation to reaction time, i.e., the time elapsed between the relatively rapid presentation of a stimulus and the behavioral response 73. This result is similar to those of a systematic review conducted by Wang et al. 74, as it also recognizes that Baduanjin training benefits people with stroke in several domains, such as global cognitive function, including memory and executive functions. However, it did not find any significant difference in attention. In combinations involving physical resistance activity, all three studies reported cognitive improvements in the experimental group compared to the control group 30,50,63. For studies that performed aerobic physical activity combinations, six out of eight reported improvements in the experimental group compared to the control group 29,54,58,59,62,66. A similar situation to the one presented above is also noted for the memory domain, as neither group reports significant differences in memory 40. This study rightly points to the lack of improvement seen in the memory domain, taking into account the duration of the intervention program (8 months), as it explains that cardiorespiratory fitness and memory require a more extended intervention, where fitness values must be high for exercise to induce physiological changes 40. This finding is supported in the literature, as studies have shown that most motor recovery is almost completed within 10 weeks after stroke 75, while neuronal recovery can occur within weeks or even years 76. Some studies did not record improvements in strength combinations. We believe this is due to the methodology chosen 46, as the rehabilitation program occurred at home and data were self-reported. One of the problems that negatively affects the practice of post-stroke physical activity has to do with the fear of falls, which generates a vicious cycle that leads to intolerance to physical activity, in addition to not helping to overcome post-stroke fatigue that is often experienced in patients with stroke 71,75. Therefore, the successful implementation of a physical activity program at home must be accompanied by motivational strategies that might help to increase the motivational rate 77-79. As for another study 64, it is suggested that the lack of improvements results from the fact that the participants have mild cognitive impairment (MoCA scores of 24.9 ± 3.2 for the experimental group and 25.5 ± 2.9 for the control group), associated with the relatively young age of the participants (average age of participants of 64.30 years). Another study further confirms that the benefits resulting from rehabilitation for mild cognitive deficits may be low 70.
Regarding the study that involved the combination of aerobic physical activity 65, we believe that the lack of cognitive improvement verified after the rehabilitation training program that aimed to improve cognitive deficits is associated with adherence problems. Adherence was low since three in five participants did not attend the sessions. Evidence shows that the degree of commitment strongly influences clinical findings since adherence to a physical activity program improves post-stroke recovery 79,80.
Regarding the isolated rehabilitation training program, where the predominance of aerobic physical activity was notorious, nine of the 11 studies registered cognitive improvements in the experimental group compared to the control group, and three did not report gains. The explanation for the lack of improvement is possibly linked to the heterogeneity of the study participants 49, as both patients with ischemic and hemorrhagic stroke were included, subacute to chronic patients were also included, and there was also a disparity between the ages of the participants (18-75 years). A change in the study methodology carried out at 6 months and then at 18 months after onset, associated with the type of intervention, i.e., high-intensity physical activity performed at home 39, might also explain the lack of improvements. It is possible that, in the face of high-intensity physical activity that occurs at home, stroke survivors become highly anxious about the risk of a new event. This fact can lead to fear or lack of desire to practice physical activity 75,81. Furthermore, the lack of improvements verified 57 might be due to the extensive duration of intervention, as the literature reports that the most significant gains in post-stroke recovery occur in the first 3 months 75,76,81.
Our results align with previous studies, demonstrating that combined training programs promote significant improvements in several domains, such as attention, memory, language, orientation, visuospatial ability, and executive functions, compared to isolated training programs 6,80-82. Since patients with stroke present cognitive problems 83, they should participate in combined rehabilitation programs.
Regarding the duration of rehabilitation training programs, it is essential to understand what predicts the effectiveness of exercise, as it can guide clinicians on how to better design exercise programs for people with stroke, as programs lasting less than 8 weeks are not long enough to elicit noticeable cognitive gains 84. A moderator-effect analysis revealed that the 12-14-week exercise interventions are associated with the most significant magnitude of cognitive gains 85. These results reinforce the need to use relatively long programs to rehabilitate people with stroke 85-88. However, contradictions persist regarding the duration that best optimizes cognition, as seen in a recent review where the analysis showed no difference between using a program of more than 12 weeks or less 89. This information is essential as it impacts doctors’ decisions. When relating the lack of improvements with intensity, the influence of low intensity is noted, as one study presented low-intensity physical activity 65. In another, the intensity was gradually increased 64. We suggest that the intensity of physical activity may have been too low, which failed to create physiological changes that led to the awakening of neuronal plasticity 78,85.
Regarding the studies contemplating high-intensity physical activity 48,57, we think that given the fear of falling and the risk of a new stroke event 75,76, this fact may have led to adherence problems from the perspective of adequately taking advantage of physical activity sessions 80. The study with the most extended duration used an isolated rehabilitation training program lasting 18 months. Interestingly, the two studies lasting longer than 1 year and the one lasting 18 months did not register improvements. As Yang and Wang 85 explain, when the exercise program goes beyond 14 weeks, the previously acquired cognitive benefits disappear again. This may indicate that longer-term rehabilitation training programs are poorly tolerated by patients with stroke since the time course after stroke is characterized by more significant improvements during the first few weeks after stroke. This might reflect the concomitant intrinsic pressure known as “neurological recovery” 90-93.
Two very recent meta-analyses by Yang and Wang 84,85 also consolidate this idea of long-term exercise (exercise programs for 12 weeks) because it explains that the cycle of intervention with exercise after stroke is mainly controlled at 12 weeks since this period has good patient tolerance, as well as potentiation of long-term effects on physical and mental health, and further explains that 8 weeks of post-stroke aerobic training is more or less the ideal period to have a positive impact on cardiopulmonary and cognitive function 85.
Concerning exercise intensity, in the studies reviewed here, there is a predominance of moderate-intensity physical activity; this fact seems to result from the need to safeguard the health of the participants (patients with stroke), as post-stroke exercise recommendations include moderate-intensity continuous cardiovascular exercise with a suggested intensity of 40-70% maximum oxygen consumption or heart rate reserve of 50-80% of the maximum heart rate 94-96. On the other hand, it is possible that higher-intensity exercises were not chosen because evidence indicates that high-intensity physical activity does not generate greater cognitive gain 85. However, this is a controversial position, as studies show that intensity only mediates domains of gain 97.
It is important to emphasize that previous reviews offer relatively little information about the ideal prescription of physical exercises for cognitive health. There is still no clarity in most guidelines on the methodology, essentially in terms of the frequency with which physical activity should be performed, the time that the rehabilitation program should last as well as the activity that should be performed 98; little is discussed about the need to adapt exercise based on an individual’s skill level, mobility, basic fitness level. However, a review 80,99 states that at least 30 min of moderate-intensity physical exercise five times a week for at least 150 min can be efficient. However, it is essential not to forget that post-stroke physical activity is not risk-free 98,100, so before starting physical activity, patients with stroke should go through a medical assessment to identify medical conditions that require special consideration or constitute a contraindication 100.
The results of this review further reinforce the underlying idea that physical activity benefits post-stroke physical and cognitive recovery, a fact that supports the need to prescribe physical activity as a therapy in the treatment of patients with stroke, as it can be safe, efficient, and allow the patient with stroke to adhere to a less sedentary lifestyle resulting from their pathology 75,76. Regarding the severity of the stroke, although the results of this review show that 16 of the 34 studies involved participants with chronic stroke, these data do not seem to have had a negative influence on cognitive performance because of the 34 studies included, of which 27 reached the purpose to reduce the post-stroke cognitive impairments after a rehabilitative training program. Of the seven studies that do not improve, four pertain to subacute stroke occurring within a month, and the lack of improvement might be associated with inadequacy of the intensity of the training programs, as exercise intensity should be monitored to ensure that it is strong enough to promote relevant physiological changes 81.
Although domain-level judgments provide the basis for a general assessment of the risk of bias 101,102, and based on this rationale, we refer that, in general, there is no high risk of bias since most of the evaluated studies presented a low risk of bias; having given evidence on the effectiveness of a combined rehabilitation training program, moderate intensity, with a frequency of three times a week and duration of the program of 12 weeks, caution is needed when interpreting these results. The Cochrane tool for risk of bias led us to analyze the risk as not high. However, this must be interpreted cautiously because the ten included studies present concerns in the first and second domains, which denote problems with randomization 102. We must also interpret these results cautiously since we systemized relatively few studies. These involve diverse neuropsychological instruments used to assess cognitive deficits since a variety of neuropsychological tests in use present one or more deficiencies linked to reliability or validity, standardization, lack of alternative forms, and lack of ecological validity 103.
Limitations of This Study
The present study provides an updated and extensive qualitative overview of the literature on the most effective rehabilitation training program to be used in the cognitive rehabilitation of patients with stroke. Our findings largely align with previous results that synthesized evidence on the effectiveness of post-stroke activity 78.
The major limitation of this study lies in the fact that it included methodologically heterogeneous studies, which made it difficult to compare the data, limiting the synthesis of the results. Heterogeneity was found concerning the sample, the duration of rehabilitation programs, the intensity of physical activity, the frequency with which sessions occurred, the severity of patients, and the diversity of neuropsychological tests used. In the future, these issues should be addressed, and given an array of more homogeneous studies, a meta-analysis might be an option, as it allows for transparent decisions supported by statistical analyses that help to limit biases 104.
Conclusion
This systematic review suggests that cognitive performance may improve more in people with stroke after combined rehabilitation training programs compared to rehabilitation training programs alone. This improvement seems to result from the synergistic effect of physical activity, which may be beneficial for the quality of life of this clinical group.
Recommendations
Physical activity for people with stroke should be preceded by a few precautions and guidelines:
For people with stroke, before starting physical activity, they should undergo a medical assessment to rule out or identify medical conditions that require special attention, as well as those that could be aggravated by physical activity.
The practice of physical activity for people with stroke should consider the principle of gradualism on an individual basis since cardiovascular fitness, essential in reducing the risk after stroke, is gradually achieved with regular physical activity.
The frequency, duration, and intensity of the physical activity session must be gradual to minimize adverse events and make it safe and motivating. A rehabilitation training program for people with stroke should combine different physical activities (e.g., aerobic and strength exercise, or aerobic, strength and endurance, or aerobic and cognitive training) to take more significant advantage of their synergistic action. The intensity with which each session is performed must be moderate enough to promote physiological changes that lead to cognitive optimization of physical activity.
Acknowledgments
We would like to kindly thank João Dias and Claúdia Catanho, Science Managers at UCP, for their collaboration in the protocol phase.
Statement of Ethics
This systematic review and its protocol were registered in the international prospective review registry (PROSPERO) under the registration number CRD42021248533.
Author Contributions
R.M. collected the data, developed the first draft of the manuscript, and extracted the studies. A.M.A. reviewed the first and subsequent versions and untied selection decisions. I.S.M. and R.M. decided which studies to include. I.S.M. and A.M.A. suggested improvements across all phases of the manuscript elaboration. All authors approved the final manuscript.

